Craniocervical Instability: Causes, Symptoms, Mechanisms, Testing, and How To Improve It
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Craniocervical Instability (CCI) is a structural condition in which the ligaments connecting the skull to the upper cervical spine lose their ability to hold the junction stable, allowing excessive movement that can compress the brainstem, obstruct cerebrospinal fluid flow, and kink the vertebral arteries.
In this post, we will discuss the basics of CCI, what causes it, how the craniocervical junction works, overlapping conditions (POTS, MCAS, EDS, Chiari, ME/CFS), how to improve it, what to avoid, testing and imaging, mechanisms of action, relevant genetics, and recent research.

1. Basics Of Craniocervical Instability
Craniocervical Instability (CCI) refers to excessive movement at the junction between the skull (occiput) and the first two cervical vertebrae (C1 and C2). R
This region is called the craniocervical junction (CCJ), and it is one of the most mobile and structurally vulnerable areas in the entire spine. R
The CCJ relies almost entirely on ligaments (rather than interlocking bone) for stability. R
When those ligaments become lax, damaged, or structurally inadequate, the skull can translate or rotate beyond normal limits on top of the spine. R
This excess motion can compress the brainstem, obstruct cerebrospinal fluid (CSF) flow, and compromise the vertebral arteries. R
CCI is increasingly recognized in people with Ehlers-Danlos Syndrome (EDS) and other connective tissue disorders, but it also occurs after trauma, infection, and inflammatory disease. R
Common symptoms of CCI include:
- Balance problems and gait instability
- Brain fog and cognitive difficulties
- Chronic headaches (especially occipital, worsened by neck movement)
- Difficulty swallowing (dysphagia)
- Dizziness and vertigo
- Facial pain or numbness
- Fatigue (often severe)
- Muscle weakness in arms and legs
- Nausea
- Neck pain and suboccipital pain
- Sleep disruption and frequent night awakenings
- Speech difficulties
- Syncope and pre-syncope
- Tinnitus (see tinnitus)
- Visual disturbances (blurred vision, double vision, photophobia)
The hallmark of CCI is that many of these symptoms are positional, meaning they worsen or improve depending on the position of the head and neck. R
CCI is underdiagnosed because standard supine MRI often misses the instability that becomes apparent only when the patient is upright and gravity loads the joint. R
2. What Causes Craniocervical Instability
CCI results from anything that weakens the ligamentous or bony structures of the craniocervical junction.
Connective Tissue Disorders
Ehlers-Danlos Syndrome (EDS), particularly the hypermobile subtype (hEDS), is the most recognized cause of CCI. R
In EDS, genetic defects in collagen and extracellular matrix proteins lead to ligament laxity throughout the body, including the critical ligaments at the CCJ. R
Other connective tissue disorders that increase CCI risk include Marfan syndrome, Loeys-Dietz syndrome, and osteogenesis imperfecta. R
For more on connective tissue disorders, see the Junction Dysfunction chapter on connective tissue disorders.
Trauma
Whiplash injury is a common cause of ligament damage at the CCJ, particularly to the alar ligaments and transverse ligament. R
Motor vehicle accidents, sports injuries, falls, and concussions can all produce sufficient force to stretch or tear the upper cervical ligaments. R
In people with pre-existing connective tissue laxity, even minor trauma can be enough to destabilize the joint. R
Inflammatory and Infectious Causes
Rheumatoid arthritis (RA) is the most common inflammatory cause of craniocervical instability, with 40 to 85% of RA patients showing atlantoaxial involvement. R
Chronic inflammation erodes the transverse ligament and bony structures, leading to progressive instability. R
Upper respiratory tract infections (both bacterial and viral) have been identified as triggers for atlantoaxial subluxation, either through direct inflammation spreading to the joint or through hematogenous spread. R
COVID-19 has also been reported as a cause of atlantoaxial subluxation. R
Congenital and Developmental
Down syndrome has one of the highest rates of atlantoaxial instability, present in approximately 10 to 20% of individuals, due to congenital ligamentous laxity. R
Congenital anomalies of the odontoid process (os odontoideum, aplasia of the dens) can also cause instability. R
Matrix Metalloproteinase Overactivation
Matrix metalloproteinases (MMPs) are enzymes that degrade collagen and other extracellular matrix proteins. R
When MMP activity is chronically elevated (as occurs in chronic inflammation, mast cell activation, and infection), the ligaments of the CCJ can be progressively degraded. R
See the Junction Dysfunction chapter on extracellular matrix remodeling for more on this.
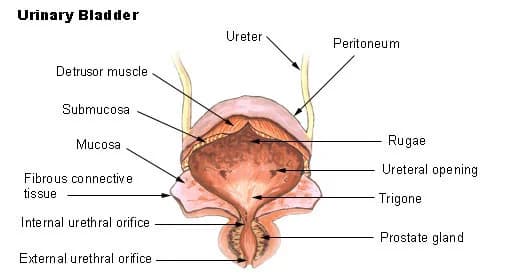
3. How The Craniocervical Junction Works
The craniocervical junction (CCJ) consists of the occiput (C0), the atlas (C1), and the axis (C2). R
This is the most mobile segment of the spine, responsible for approximately 50% of total cervical rotation and a significant portion of flexion and extension. R
C0-C1 (Atlanto-Occipital Joint)
The atlanto-occipital joint connects the skull to C1 (the atlas).
It primarily allows flexion and extension (the "yes" motion). R
The occipital condyles sit in shallow cups on the lateral masses of C1, and the joint capsules, tectorial membrane, and alar ligaments provide stability. R
C1-C2 (Atlantoaxial Joint)
The atlantoaxial joint is the primary rotation joint of the cervical spine, accounting for roughly 50% of total head rotation. R
C2 has a unique bony projection called the odontoid process (dens) that projects upward through the ring of C1. R
The dens acts as a pivot point, and the transverse ligament wraps around it posteriorly to prevent anterior translation. R
Critical Ligaments
Transverse ligament: The strongest and most important ligament at the CCJ, spanning between the lateral masses of C1 and wrapping behind the dens. R
It prevents the dens from translating posteriorly into the spinal cord. R
The transverse ligament averages approximately 22 mm in length and is the primary restraint against anterior atlantoaxial subluxation. R
Alar ligaments: These paired ligaments connect the tip of the dens to the medial aspect of the occipital condyles. R
They limit rotation and lateral bending of the head, and they average approximately 10 mm in length. R
The alar ligaments also have a lower portion that attaches to the lateral masses of C1, providing additional stability. R
Tectorial membrane: A continuation of the posterior longitudinal ligament that covers the dens and transverse ligament, adding a secondary layer of support. R
Apical ligament: A small midline ligament connecting the tip of the dens to the anterior margin of the foramen magnum. R
What Passes Through The CCJ
The brainstem (specifically the medulla oblongata) transitions into the upper spinal cord at this level. R
The medulla oblongata contains the nuclei for autonomic function, including cardiovascular regulation, respiratory drive, and the vagus nerve (cranial nerve X). R
The vertebral arteries ascend through the transverse foramina of C1 and C2 before entering the skull to supply the brainstem and posterior brain. R
Cerebrospinal fluid (CSF) circulates through the foramen magnum, and any obstruction at this level can impair drainage and flow. R
The inferior ganglion (nodose ganglion) of the vagus nerve sits directly anterior to C1, and the superior cervical sympathetic ganglion lies anterior to C2 and C3, making both exquisitely vulnerable to compression and traction from instability. R
4. Craniocervical Instability And Overlapping Conditions
CCI rarely exists in isolation.
It shares significant overlap with a cluster of conditions that are now recognized as a common triad (and sometimes pentad) in connective tissue disorders.
Ehlers-Danlos Syndrome (EDS)
EDS is a group of heritable connective tissue disorders caused by defects in collagen and extracellular matrix proteins. R
The hypermobile subtype (hEDS) is the most common type associated with CCI. R
In a surgical series of 20 CCI patients with connective tissue disorders, 10 had hEDS, 2 had classical EDS, 4 had unspecified EDS, and 4 had hypermobility spectrum disorder. R
For more on how connective tissue disorders develop, see the Junction Dysfunction chapter on connective tissue disorders.
Postural Orthostatic Tachycardia Syndrome (POTS)
POTS is a form of dysautonomia characterized by an excessive heart rate increase upon standing.
CCI can cause POTS through brainstem compression of the autonomic regulatory centers in the medulla oblongata. R
Compression of the vagus nerve and superior cervical sympathetic ganglion at the C0-C2 level provides a direct mechanical mechanism for the dysautonomia seen in many CCI patients. R
In the Henderson surgical series, orthostatic grading scores improved significantly after craniocervical fusion. R
See the Junction Dysfunction chapter on vascular POTS for more on the vascular mechanisms.
Mast Cell Activation Syndrome (MCAS)
Mast cell activation and CCI are linked bidirectionally.
MCAS is clinically associated with both POTS and EDS as part of the recognized triad. R
Mast cell-derived enzymes, including tryptase and matrix metalloproteinases, can degrade the collagen in cervical ligaments, potentially contributing to the development of CCI. R
Conversely, brainstem compression from CCI can dysregulate the autonomic nervous system, which in turn modulates mast cell degranulation. R
For more on the mast cell and glial cell interaction, see mast cell-glia interactions.
Chiari Malformation Type I
Chiari Malformation Type I (CM1) involves herniation of the cerebellar tonsils through the foramen magnum. R
CM1 and CCI frequently co-occur, particularly in patients with EDS. R
CCI may worsen tonsillar herniation by destabilizing the foramen magnum, and CM1 decompression surgery sometimes unmasks underlying CCI that was previously compensated. R
Both conditions can independently obstruct CSF flow and compress the brainstem. R
Tethered Cord Syndrome
Tethered cord syndrome (TCS) involves abnormal attachment of the spinal cord at the caudal end, restricting its normal movement within the spinal canal. R
TCS co-occurs with both CCI and CM1 in patients with hEDS, suggesting a shared connective tissue mechanism across the entire neuraxis. R
Caudal traction from a tethered cord may exacerbate cranial settling and brainstem compression at the CCJ. R
Intracranial Hypertension
Intracranial hypertension (IH) involves elevated pressure within the skull, presenting with headache, visual changes, pulsatile tinnitus, and cognitive symptoms. R
CCI can contribute to IH by compressing the internal jugular veins at the craniocervical level, impairing venous outflow from the brain. R
Because the cranio-vertebral venous system lacks valves, any obstruction to venous outflow is directly reflected in CSF pressure. R
Myalgic Encephalomyelitis / Chronic Fatigue Syndrome (ME/CFS)
A landmark study by Bragee et al. found that 80% of ME/CFS patients had craniocervical obstructions on cervical MRI, and 83% had signs of intracranial hypertension. R
Hypermobility was identified in 50% of the 229 ME/CFS patients in that cohort. R
This suggests that a subset of ME/CFS patients may have a mechanical basis for their symptoms. R
For more on the inflammatory component, see SALI (systemic and long-term inflammation) and the Cell Danger Response.
Body Buzzing and Internal Tremors
Many CCI patients report body buzzing and internal tremors, which may result from compression of the descending motor pathways and proprioceptive tracts at the cervicomedullary junction.
See the Junction Dysfunction chapter on Wallerian degeneration for more on the mechanism.
Trigeminal Neuralgia
Trigeminal neuralgia is a chronic neuropathic pain condition that produces electric shock-like facial pain.
The trigeminal nerve nucleus (specifically the spinal trigeminal nucleus) extends from the brainstem down into the upper cervical spinal cord at C1-C3, placing it directly in the zone of mechanical compression from CCI. R
Brainstem compression at the cervicomedullary junction can sensitize this nucleus, lowering the threshold for trigeminal pain attacks even without classical neurovascular compression. R
CCI patients who develop facial pain, particularly pain that worsens with head position changes, should be evaluated for trigeminal involvement.
5. How To Improve Craniocervical Instability
Management of CCI ranges from conservative approaches to surgical intervention, depending on severity and the degree of neurological compromise.
Physical Therapy and Neuromuscular Training
Specialized physical therapy focusing on cervical stabilization and proprioceptive retraining is the foundation of conservative CCI management. R
Craniocervical flexor (CCF) training targets the deep neck flexor muscles (longus colli, longus capitis) that directly stabilize the upper cervical spine. R
International expert consensus recommends beginning with isometric holds and only gradually progressing to controlled cervical movement, avoiding any exercise that causes symptom exacerbation. R
Key elements of the physical therapy approach include:
- Breathing pattern correction (diaphragmatic breathing)
- Deep cervical flexor activation and endurance training
- Gradual cervical proprioceptive exercises (laser pointer retraining)
- Isometric cervical stabilization in neutral
- Postural correction (addressing forward head posture)
- Scapular stabilization exercises
Prolotherapy and Regenerative Injections
Prolotherapy involves injection of a proliferant solution (typically dextrose) at ligament attachment sites to stimulate an inflammatory healing response and strengthen lax ligaments. R
Fluoroscopically guided cervical prolotherapy has shown statistically significant reductions in both cervical flexion/extension translation and pain scores. R
Platelet-Rich Plasma (PRP) injections deliver supraphysiological concentrations of growth factors (PDGF, VEGF, TGF-beta, IGF) to the injection site to accelerate ligament healing. R
PRP has been shown to improve spinal ligament healing through activation of inflammatory and regenerative pathways. R
For more on VEGF and TGF-Beta1, see those respective posts.
Cervical Collar / Orthosis
A rigid cervical collar (such as an Aspen Vista collar) can provide external stabilization and symptom relief while rehabilitative or regenerative treatments take effect.
Collar use should be temporary and combined with active rehabilitation, because prolonged immobilization leads to cervical muscle atrophy, which can worsen instability long-term. R
Supplements for Connective Tissue Support
The following supplements support collagen synthesis, ligament integrity, and connective tissue repair:
- BPC-157 promotes tendon and ligament healing through enhanced fibroblast proliferation, collagen synthesis, and FAK-paxillin signaling R (see BPC-157)
- Collagen Peptides (Type I and III) provide the amino acids glycine, proline, and hydroxyproline, which are direct precursors for collagen synthesis in ligaments R
- Copper is the essential cofactor for lysyl oxidase, the enzyme that crosslinks collagen and elastin fibers R (see zinc/copper)
- Creatine supports cellular energy, brain function, and has neuroprotective properties relevant to brainstem compression creatine
- GHK-Cu stimulates collagen synthesis, activates tissue remodeling genes, and promotes wound healing GHK-Cu
- Lion's Mane promotes nerve growth factor (NGF) production, supporting neuroregeneration in the context of nerve compression Lion's Mane (see also NGF)
- Palmitoylethanolamide (PEA) reduces neuroinflammation and mast cell activation, addressing the inflammatory component of CCI PEA/Luteolin
- Vitamin C is an essential cofactor for both prolyl hydroxylase and lysyl hydroxylase, enzymes required for proper collagen triple-helix formation R (see vitamin D cofactors)
- Vitamin C + Gelatin Protocol taken together 1 hour before exercise can double collagen synthesis rates compared to exercise alone R
- Zinc supports MMP regulation, immune function, and connective tissue repair (see zinc/copper balance and mineral balancing)
Additional supportive supplements:
- CBD for pain and neuroinflammation management (see CBD/THC)
- Low Dose Naltrexone (LDN) for neuroinflammation and pain modulation (see LDN)
- Melatonin for sleep disruption and neuroprotection (see melatonin)
- NAD+ Precursors (NMN/NR) for mitochondrial support and neuronal energy (see NAD+/NADH)
- Theanine for anxiety and excitotoxicity (see theanine)
Surgical Intervention: Occipitocervical Fusion
Occipitocervical fusion (OCF) is the surgical treatment for severe CCI that has failed conservative management. R
OCF involves fusing the occiput to C2 (and sometimes C3) using screws and rods to eliminate pathological motion. R
In the Henderson series of 20 EDS patients who underwent craniocervical reduction and fusion, statistically significant improvements were demonstrated for headache, neck pain, nausea, syncope, speech difficulties, concentration, vertigo, dizziness, numbness, arm weakness, and fatigue at 5-year follow-up. R
A larger series of 53 EDS patients showed that OCF significantly improved pain, cranial nerve deficits, cervical medullary syndrome, and myelopathic symptoms. R
Fusion rates approach 100% in modern series, though patients with EDS may have higher rates of complications including hardware failure due to poor bone and tissue quality. R
OCF is a permanent procedure that eliminates motion at the fused segments, so it is reserved for cases with documented neurological compromise or severe symptoms unresponsive to conservative treatment. R
6. What To Stay Away From
If you have CCI (or suspect it), the following should be avoided or approached with extreme caution:
- Cervical chiropractic manipulation (HVLA thrusts): High-velocity, low-amplitude adjustments to the upper cervical spine can worsen ligament laxity and increase subluxation risk in an already unstable joint
- Excessive neck flexion/extension: Looking straight down at a phone for extended periods (forward head posture) or extreme neck extension increases mechanical stress on the CCJ R
- Headstands, inversions, and yoga poses that load the cervical spine: These place the full body weight through an unstable CCJ
- Heavy overhead lifting: Axial compression with rotation can exacerbate instability
- High-impact activities: Contact sports, roller coasters, trampolines, and other activities that produce jarring cervical forces
- Ignoring symptom patterns: If symptoms consistently worsen in specific head positions, that positional correlation is diagnostically important and should be documented for your provider
- Prolonged collar use without rehabilitation: Extended immobilization weakens the cervical muscles, creating a dependency cycle R
- Supine-only imaging: A normal supine MRI does not rule out CCI, because gravity-dependent instability is only captured in upright or dynamic studies R
7. Testing
CCI diagnosis requires specialized imaging, because standard supine MRI frequently misses dynamic instability.
Upright MRI
Upright dynamic MRI (udMRI) is considered the most informative imaging modality for CCI. R
Unlike conventional supine MRI, upright MRI captures the craniocervical junction under gravitational load and allows imaging in flexion, extension, and neutral positions. R
A study comparing upright and supine imaging in healthy subjects found significant differences in radiographic indicators between positions, confirming that supine imaging alone is insufficient. R
Key Radiographic Measurements
The four most commonly used diagnostic measurements for CCI are: R
Clivo-Axial Angle (CXA) / Basion-Axial Angle (BAA): Measured between the clivus and the posterior body of C2.
Normal CXA is approximately 155 degrees, decreasing approximately 10 degrees in flexion and increasing approximately 10 degrees in extension. R
A CXA less than 135 degrees has traditionally been considered pathological (indicating brainstem kyphosis), although recent reference range data suggests this cutoff may lead to overdiagnosis. R
The CXA specifically indicates the degree of ventral brainstem deformity. R
Grabb-Oakes Line (pB-C2): The perpendicular distance from the dura to a line drawn from the basion to the posterior-inferior C2.
Values greater than 9 mm have been used to indicate ventral brainstem compression, although 6 to 14% of healthy subjects exceed this threshold depending on position. R
Updated reference ranges are 4.2 to 10.2 mm at neutral, 3.8 to 10.6 mm in flexion, and 2.7 to 9.1 mm in extension. R
Basion-Dens Interval (BDI) / Vertical Harris Measurement: The distance from the basion to the tip of the dens.
Normal BDI is less than 12 mm, with values exceeding this suggesting occipital-cervical dissociation. R
Basion-Axial Interval (BAI) / Horizontal Harris Measurement: The horizontal distance from the basion to the posterior axial line.
Normal BAI is less than 12 mm. R
Digital Motion X-Ray (DMX)
Digital Motion X-ray (DMX) captures real-time video fluoroscopy of the cervical spine during active movement. R
DMX can reveal dynamic instability patterns that static imaging misses, including excessive translation and angular motion during active flexion, extension, and rotation. R
CT Imaging
CT provides excellent visualization of the bony anatomy (odontoid morphology, fractures, bony erosions) and is often used alongside MRI for surgical planning. R
CT with reconstructions can identify os odontoideum, dens aplasia, and basilar invagination. R
Lab Testing
While CCI itself is diagnosed by imaging, laboratory testing is important for identifying the underlying cause and comorbid conditions:
- Neural Zoomer for brain autoimmunity, blood-brain barrier permeability, demyelination, and neuropathy markers
- Immune Zoomer for autoantibody panels and mast cell markers
- Foundation Zoomer for CBC, CMP, thyroid, and liver function
- Nutrient Zoomer for vitamin C, copper, zinc, and other cofactors essential for collagen synthesis
- Cellular Zoomer for organic acids and mitochondrial function
- POTS Bundle (Cellular + Hormone + Gut + Neural) for comprehensive dysautonomia workup
8. Mechanisms Of Action
Simple
The core mechanism of CCI is mechanical.
When the ligaments that hold the skull to C1 and C2 become too loose, the skull moves too much relative to the spine.
This excess movement causes three problems:
- The brainstem (the control center for heart rate, blood pressure, breathing, digestion, and consciousness) gets compressed or stretched.
- The flow of cerebrospinal fluid (the protective fluid that bathes the brain and spinal cord) gets blocked, leading to pressure buildup in the skull.
- The vertebral arteries (the blood vessels that supply the back of the brain) get kinked or compressed, reducing blood flow.
These three problems together explain why CCI causes such a wide range of symptoms, from headaches and dizziness to brain fog, fatigue, POTS, vision changes, and difficulty swallowing.
The symptoms are often positional because the compression changes based on head position.

Advanced
Brainstem Compression and Autonomic Dysregulation
The ventral lateral medulla contains widely collateralized sympathetic neurons that project to preganglionic neurons at multiple spinal levels and to command neurons in the central nervous system. R
Compression of this region creates chronic focal encephalopathy, disrupting sympathetic outflow and parasympathetic tone simultaneously. R
The vagus nerve (cranial nerve X) originates from the nucleus ambiguus and the dorsal motor nucleus of the vagus in the medulla, both of which are vulnerable to compression at the CCJ. R
The inferior ganglion (nodose ganglion) of the vagus nerve lies directly anterior to C1, meaning even subtle C0-C1 instability can mechanically irritate or compress it. R
This vagal dysfunction contributes to dysautonomia, gastroparesis, tachycardia, and the sensation of air hunger reported by many CCI patients. R
Vertebral Artery Compromise
The vertebral arteries traverse the transverse foramina of C1 and C2 and make a sharp turn (the V3 segment) as they enter the skull. R
CCI can cause dynamic compression of the vertebral arteries during head rotation or extension, a phenomenon also called Bow Hunter syndrome or rotational vertebral artery syndrome. R
Vertebrobasilar insufficiency from this compression presents as transient ischemic attacks, syncope, vertigo, visual disturbances, and drop attacks. R
CSF Flow Obstruction and Intracranial Pressure
The foramen magnum is the bottleneck for CSF circulation between the cranial and spinal compartments. R
CCI can narrow this passage dynamically, creating intermittent CSF flow obstruction that produces symptoms similar to Chiari malformation even in the absence of tonsillar herniation. R
Impaired venous outflow through the internal jugular veins (which pass adjacent to C1-C2) contributes to elevated intracranial pressure through the Monroe-Kellie doctrine. R
See the Junction Dysfunction chapter on lymphatic and glymphatic systems for more on CSF dynamics.
Proprioceptive Disruption (Functional Instability)
Beyond structural instability, the upper cervical spine has the highest density of proprioceptive mechanoreceptors in the body. R
Damage to the cervical proprioceptive system creates what has been called functional craniocervical instability, in which abnormal mechanoreceptor activity produces "informational noise" that disrupts vestibular processing. R
This results in disharmony between the centers controlling eye movements, the cerebellum, spinal motor neurons, and the vestibular system, producing dizziness, nystagmus, and postural instability even when structural measurements appear borderline. R
Ligament Degradation Mechanisms
In connective tissue disorders, the molecular basis of ligament failure involves defective collagen structure.
Collagen crosslinking requires lysyl oxidase, a copper-dependent enzyme that oxidatively deaminates lysine residues to form stable covalent crosslinks between collagen fibrils. R
In inflammatory states, elevated matrix metalloproteinase (MMP) activity degrades collagen faster than it can be replaced. R
Mast cell degranulation releases tryptase and other proteases that directly degrade the extracellular matrix. R
See histamine intolerance and inflammation and wound healing cycles for more on these cascades.
Collagen Synthesis Requirements
Vitamin C (ascorbic acid) is the essential cofactor for both prolyl 4-hydroxylase and lysyl hydroxylase. R
These enzymes catalyze the hydroxylation of proline and lysine residues in procollagen, which is required for proper triple-helix folding. R
Without adequate vitamin C, the enzyme's iron center cannot be reduced from Fe(III) to Fe(II), halting collagen maturation. R
Vitamin C also stimulates collagen gene transcription independently of its hydroxylation role. R
Vitamin C combined with gelatin (15 g, taken 1 hour before exercise) doubled amino-terminal propeptide of collagen I (a marker of collagen synthesis) in serum and increased collagen content and mechanics in engineered ligaments. R
9. Genetics
CCI itself is not a single-gene disorder, but the underlying connective tissue vulnerabilities that predispose to CCI are genetically mediated.
Collagen Gene Mutations
COL5A1 and COL5A2: Mutations in these genes (encoding type V collagen alpha-1 and alpha-2 chains) are the most common cause of classical EDS, with COL5A1 haploinsufficiency found in approximately one third of classical EDS patients. R
COL3A1: Mutations in the COL3A1 gene (encoding type III collagen) cause vascular EDS, the most severe subtype, with arterial and organ fragility. R
COL1A1 and COL1A2: Mutations in type I collagen genes cause some cases of classical EDS and all cases of osteogenesis imperfecta. R
Type I collagen is the primary structural collagen of ligaments, tendons, and bone. R
Extracellular Matrix Gene Mutations
TNXB: Mutations in the tenascin-X gene cause a form of EDS with marked joint hypermobility and skin hyperextensibility. R
PLOD1: Mutations in the lysyl hydroxylase 1 gene cause kyphoscoliotic EDS, characterized by severe muscle hypotonia, progressive scoliosis, and tissue fragility. R
ADAMTS2: Mutations in the procollagen N-proteinase gene cause dermatosparaxis EDS. R
TGF-Beta Signaling Pathway
TGFBR1 and TGFBR2: Mutations in the TGF-beta receptor genes cause Loeys-Dietz syndrome, a connective tissue disorder with significant craniocervical instability risk. R
Altered TGF-beta signaling disrupts collagen maturation and vascular remodeling throughout the body. R
For more on TGF-beta, see TGF-Beta1 modulation.
Hypermobile EDS (hEDS)
hEDS is the most common EDS subtype associated with CCI, but its genetic basis remains unidentified. R
hEDS is diagnosed clinically (using the 2017 criteria), and no single causative gene has been identified despite extensive sequencing efforts. R
This suggests hEDS may be polygenic or involve regulatory variants not captured by standard gene panel testing. R
For more on genetic testing related to connective tissue, see the Methylation Genetics test.
For more on methylation, see that post.
10. More Research
CCI research is rapidly evolving, and several areas of active investigation are relevant.
Diagnostic Standardization
A systematic review found a lack of consensus on diagnostic imaging parameters for CCI in EDS, with ten different radiographic parameters reported across studies and no universally accepted cutoff values. R
Recent work establishing reference ranges for the four main CCI measurements using upright dynamic MRI in healthy subjects is a significant step toward standardization. R
Some existing cutoff values (particularly the CXA less than 135 degrees threshold) may lead to overdiagnosis, and updated reference ranges are needed for clinical application. R
Non-Surgical Management
A case series demonstrated that non-surgical management of upper cervical instability through improved cervical lordosis (using specific chiropractic corrective techniques, not HVLA thrusts) produced measurable improvements in cervical alignment and symptoms. R
International expert consensus on physical therapy management of upper cervical instability in patients with generalized joint hypermobility was published in 2023, providing the first evidence-based framework for conservative treatment. R
Cervicovagopathy
A newly described clinical entity called cervicovagopathy proposes that ligamentous cervical instability causes vagus nerve dysfunction through mechanical compression and traction at the C0-C2 level. R
This framework connects CCI directly to the dysautonomia, gastroparesis, and other vagal symptoms reported by patients. R
ME/CFS Connection
The Bragee et al. study finding 80% craniocervical obstructions and 83% intracranial hypertension signs in ME/CFS patients has opened a new line of investigation into whether a subset of ME/CFS has a treatable structural cause. R
A proposed paradigm suggests that ME/CFS exists on a spectrum between idiopathic intracranial hypertension and spontaneous intracranial hypotension, both potentially caused by cranial venous outflow obstruction at the cervical level. R
Functional vs. Structural Instability
Recent research differentiating structural CCI from functional CCI proposes that proprioceptive damage at the CCJ can produce CCI-like symptoms even without measurable ligament laxity. R
Functional instability may explain why some patients have severe symptoms with borderline imaging findings, and why proprioceptive retraining can improve symptoms in the absence of measurable structural change. R
Surgical Technique Advances
Comparison of occipital bone fixation versus occipital condyle fixation in CCI patients with EDS showed that occipital condyle fixation may provide improved construct rigidity with lower failure rates. R
Newer biomechanical approaches to occipitocervical fusion are being developed to address the unique challenges of operating on patients with inherently defective connective tissue. R
Ligamentous Cervical Instability as a Disease Etiology
A comprehensive 2024 review proposed that ligamentous cervical instability from modern forward-head posture and face-down device use is an underrecognized etiology of multiple human diseases, through obstruction of fluid flow into and out of the brain. R
This framework connects CCI to a broader spectrum of neurological and systemic diseases through impaired CSF and venous circulation. R
For more on related inflammatory and structural mechanisms, see the following:
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Electrolyte Complex
1 scoop/day
CoQ10
200mg/day
Magnesium Glycinate
400mg at bedtime