Creatine: Benefits, Dosing, Brain Health, And What The Research Actually Shows
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Creatine is the most studied ergogenic supplement in existence, and yet most people still think of it only as a muscle supplement while missing its substantial and increasingly well-documented effects on the brain.
In this post, we will discuss what creatine is, how it works, the full range of evidence-based benefits including muscle, brain, mood, and neuroprotection, natural food sources, how to dose it, what to avoid, and the genetics that make some people respond far more dramatically than others.

What Is Creatine
Creatine is a nitrogenous organic acid synthesized endogenously from three amino acids: arginine, glycine, and methionine. R
The synthesis occurs in a two-step process: AGAT (arginine:glycine amidinotransferase) in the kidney converts arginine and glycine to guanidinoacetate (GAA), and GAMT (guanidinoacetate N-methyltransferase) in the liver methylates GAA to produce creatine, using SAM-e as the methyl donor. R
From the liver, creatine enters circulation and is taken up into tissues via the creatine transporter SLC6A8, a sodium- and chloride-dependent solute carrier expressed at highest levels in skeletal muscle and kidney. R
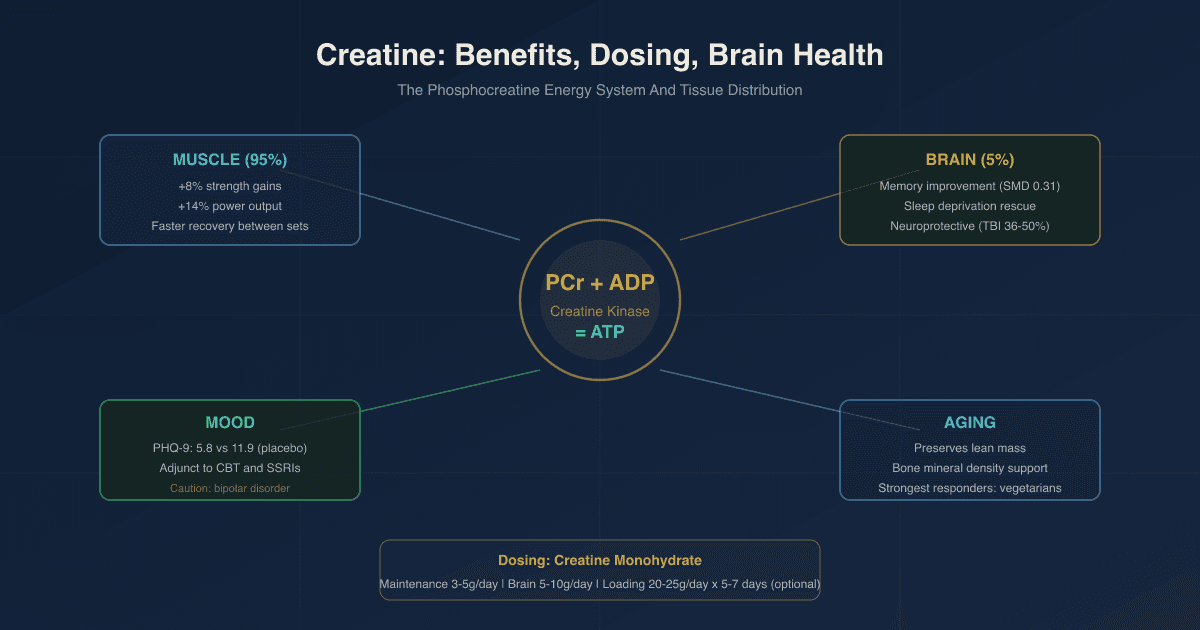
Approximately 95% of the body's total creatine is stored in skeletal muscle as either free creatine or phosphocreatine (PCr). R
The brain holds roughly 5% of total body creatine, and that 5% is disproportionately important for neurological function given the brain's extraordinary energy demands.
The total creatine pool in an average 70kg person is approximately 120-140g, with an endogenous synthesis rate of 1-2g per day and a dietary intake requirement of another 1-2g per day (from meat and fish) to maintain adequate stores. R
Vegetarians consistently have lower muscle and brain creatine levels because they consume essentially no dietary creatine, making them the population that responds most dramatically to supplementation. R
Benefits Of Creatine
1. Muscle Strength And Power Output
This is the evidence base no one disputes.
Creatine supplementation combined with resistance training consistently increases muscle phosphocreatine stores, improving ATP resynthesis during high-intensity exercise. R
The practical results: more reps per set, more power output, greater strength gains, and faster recovery between high-intensity efforts.
A meta-analysis of over 70 studies found that creatine supplementation produces approximately 8% greater strength increases and 14% greater power output increases compared to placebo alongside resistance training. R
These effects are consistent across populations: young athletes, older adults, males and females, trained and untrained individuals.
The effect is strongest in activities requiring repeated bursts of maximal effort (sprinting, weightlifting, HIIT) and less relevant to continuous submaximal endurance work (long-distance running).
2. Muscle Mass And Body Composition
Creatine increases intramuscular water content (creatine is osmotically active), increases cell volume, and through this volumizing effect may signal anabolic pathways. R
Long-term creatine supplementation with resistance training produces greater lean mass gains compared to resistance training alone.
Creatine also reduces muscle atrophy during immobilization and rehabilitation periods, making it clinically useful during injury recovery. R
3. Cognitive Function And Memory
This is the benefit most people are not aware of, and the evidence has strengthened substantially over the past decade.
A 2024 systematic review and meta-analysis of RCTs found that creatine supplementation significantly improved memory (SMD = 0.31, p less than 0.00001), and showed positive effects on attention and information processing speed. R
The cognitive effects appear strongest in three specific contexts: R
- Sleep deprivation: A 2024 Nature Scientific Reports study using a high single dose (0.35g/kg) during sleep deprivation demonstrated measurable changes in cerebral high-energy phosphates (ATP/PCr ratio) alongside improved cognitive performance on multiple tasks. R
- Aging: Older adults, who have lower baseline brain creatine levels, show more consistent cognitive improvement from supplementation than young healthy adults. R
- Vegetarians: Those with the lowest baseline creatine stores show the largest cognitive gains because they have more room to fill. R
The magnitude of cognitive benefit from creatine in well-rested, meat-eating young adults is modest and inconsistent across studies. R
This is an honest reading of the literature. Creatine is not a stimulant. It supports energy substrate availability in the brain and that benefit is most detectable when energy availability is otherwise compromised.
4. Depression And Mood
This is a rapidly developing area and the signal is clinically interesting. There is a MAYBE here.
Creatine concentrations in the prefrontal cortex are negatively correlated with depressive symptoms: lower prefrontal creatine, worse depression. R
A 2024 RCT found that 5g/day creatine added to cognitive-behavioral therapy (CBT) for depression produced significantly greater reductions in PHQ-9 depression scores at 8 weeks compared to CBT plus placebo (mean PHQ-9 dropped to 5.8 in creatine group vs 11.9 in placebo group). R
A 2012 RCT in women with major depressive disorder found that adding 3-5g/day creatine to escitalopram (SSRI) produced faster and greater antidepressant response compared to escitalopram plus placebo. R
A 2025 systematic review of 5 RCTs found creatine (2-10g/day for 4-8 weeks) as an adjunct to antidepressants or CBT showed consistent benefit for major depressive disorder, with good tolerability. R
There is an important caveat: one bipolar depression trial reported a manic switch in a patient taking creatine, and there are animal and case reports of increased agitation or depression-like behavior in some males taking high doses. R
Creatine for depression looks promising as an adjunct, particularly for females, treatment-resistant depression, and patients with low baseline creatine (vegetarians, elderly).
Use caution in bipolar disorder specifically.
5. Traumatic Brain Injury And Concussion Recovery
Animal models consistently show creatine supplementation reduces cortical damage from TBI by 36-50% when administered prior to injury. R
Human studies in children with mild TBI show improvements in cognition, communication, self-care, and reductions in headaches, dizziness, and fatigue with creatine supplementation. R
The ISSN (International Society of Sports Nutrition) position stand identifies creatine as having neuroprotective benefits relevant to concussion and spinal cord injury. R
The clinical implication: creatine may be worth maintaining prophylactically in contact sport athletes, particularly given its strong safety profile.
6. Aging And Sarcopenia
Skeletal muscle creatine content declines with age.
Older adults with lower dietary creatine intake (less than 0.95g/day) show poorer cognitive function compared to those consuming more. R
Creatine supplementation combined with resistance training reduces muscle atrophy, preserves lean mass, and may improve bone mineral density in aging populations. R
For older adults, creatine is one of the most well-supported and underutilized supplements available.
7. Post-Viral Fatigue And Long COVID
Emerging evidence suggests creatine may have a role in supporting recovery from post-viral fatigue syndromes including Long COVID, through its support of mitochondrial energy production and anti-inflammatory properties. R
This is early-stage evidence but mechanistically plausible: if mitochondrial function is compromised post-virally (as appears to be the case in Long COVID), creatine supplementation may provide an energy substrate buffer that partially compensates.
8. Bone Health
Creatine can increase osteoblast activity (bone formation) and may reduce bone resorption, particularly when combined with resistance training. R
Preliminary findings are encouraging for conditions associated with accelerated bone loss, though large-scale clinical trials confirming this are still needed.
Natural Sources Of Creatine
Creatine is found almost exclusively in animal products. R
Approximate creatine content by food (raw, per kg): (not exclusive list)
- Beef: 4.5g/kg
- Chicken breast: 3.4g/kg
- Herring: 6.5-10g/kg (one of the highest natural sources)
- Pork: 5.0g/kg
- Salmon: 4.5g/kg
- Tuna: 4.0g/kg
Cooking reduces creatine content modestly as some converts to creatinine under heat.
Plant foods contain negligible creatine, which is why vegetarians and vegans maintain lower muscle and brain creatine stores and are among the highest responders to supplementation. R
Achieving 5g/day from food alone would require approximately 1kg of raw beef daily, which is impractical.
Supplementation is the only realistic way to consistently achieve the doses used in most research.
Dosing And Forms
Form: Creatine Monohydrate First
Creatine Monohydrate is the form with the most research, the longest safety record, and the lowest cost.
Near-100% oral bioavailability. No meaningful advantage has been demonstrated for creatine HCl, buffered creatine, creatine ethyl ester, or other marketed alternatives in well-controlled trials. R
The monohydrate is not broken down in the GI tract. It is absorbed intact and enters the bloodstream efficiently.
Standard Maintenance Dosing
3-5g/day is the dose used in the majority of the cognitive and mood research, and is effective for maintaining saturated muscle and tissue stores over time. R
This is a conservative and appropriate starting point for most people.
Smaller individuals can go closer to 3g. Larger individuals or those doing high-volume training can go up to 5g.
Loading Protocol (Optional)
20-25g/day in 4-5 divided doses for 5-7 days, followed by 3-5g/day maintenance. R
Loading saturates muscle stores approximately 30% faster than maintenance dosing alone, but both approaches reach the same endpoint by around 4 weeks.
GI distress (bloating, cramping, loose stools) is more common during loading because of the high daily doses. Splitting into 4-5 small doses throughout the day rather than taking it all at once significantly reduces this.
There is no meaningful advantage to loading for most use cases. Patience and a maintenance dose achieves the same result.
Higher Doses For Brain Effects
The cognitive research uses 5-10g/day or higher for brain-specific effects, because crossing the blood-brain barrier is less efficient than loading skeletal muscle. R
Only approximately 5% of total body creatine is stored in the brain, and the blood-brain barrier limits creatine uptake from the periphery.
If the primary goal is cognitive or mood support, 5g/day is a reasonable floor and some research uses 10g for stronger effects.
Timing
The exact timing of creatine relative to exercise has modest importance.
Post-exercise ingestion may be slightly superior to pre-exercise based on limited evidence, as exercise-induced blood flow enhances muscle creatine uptake. R
Taking creatine with carbohydrates or protein further enhances muscle uptake via insulin-mediated transporter activity. R
For non-athletic cognitive or mood use, timing relative to meals matters less. Take it consistently at the same time each day.
Micronized Creatine
Micronized Creatine Monohydrate is the same molecule as regular creatine monohydrate, just milled to a smaller particle size.
This improves mixability and may reduce GI discomfort in sensitive individuals.
It is not more bioavailable than regular creatine monohydrate. It is simply easier to dissolve.
Conditions Linked To Low Creatine
Creatine Deficiency Syndromes (CDS)
Three genetic disorders cause severe brain creatine deficiency. R
All three present with the same core phenotype: intellectual disability, severe speech and language delay, seizures, movement disorders, and behavioral abnormalities including ADHD and autism spectrum features.
AGAT Deficiency (GATM gene, autosomal recessive): The first enzyme in creatine synthesis is absent or impaired. AGAT cannot convert arginine and glycine to guanidinoacetate. Brain creatine is severely depleted. Because the transporter is intact, supplemental dietary creatine can reach the brain and treatment with creatine monohydrate produces significant and sometimes remarkable recovery of function. R
GAMT Deficiency (GAMT gene, autosomal recessive): The second synthesis enzyme is absent. Guanidinoacetate accumulates (itself neurotoxic), and creatine production fails. More complex to treat than AGAT deficiency due to GAA toxicity; requires creatine supplementation plus arginine restriction and ornithine supplementation. R
SLC6A8 (CRTR) Deficiency (X-linked): The creatine transporter is mutant, preventing creatine from entering cells. Females heterozygous for the mutation show variable expression from learning disabilities to seizures. Males are fully affected. This is the second largest cause of X-linked intellectual disability after Fragile X syndrome. Oral creatine supplementation is ineffective because the problem is the transporter, not the supply of creatine; even high doses cannot enter cells normally. R
Functional Low Creatine (Non-Genetic)
Beyond the rare genetic deficits, several populations have functionally low creatine stores:
- Aging (reduced synthesis and dietary intake)
- Depression (lower prefrontal creatine is documented) R
- Post-viral fatigue and Long COVID
- Vegetarian and vegan diet
- Chronic kidney disease (impaired endogenous synthesis due to loss of AGAT activity in diseased kidneys)
What To Stay Away From
- Creatine in frank renal insufficiency (creatine converts spontaneously to creatinine at approximately 2%/day; creatinine is the primary clinical marker of kidney function; in diseased kidneys this creates a diagnostic confound; creatine is not directly nephrotoxic at standard doses in healthy kidneys, but its use in advanced kidney disease requires nephrology input) R
- High-dose creatine loading in bipolar disorder (two case reports of manic switch; caution warranted until more data is available) R
- Creatine ethyl ester (marketed as superior, but the ethyl ester bond breaks down to creatinine in the gut and plasma faster than monohydrate; studies show worse tissue retention than monohydrate) R
- Creatine with caffeine at high doses concurrently (some older evidence suggested caffeine partially antagonized creatine's ergogenic effect by altering phosphocreatine resynthesis kinetics; more recent data is less clear; the practical effect is probably minimal at typical caffeine intakes, but worth noting for high-performance athletes)
- Expecting cognitive benefits in a well-rested, well-nourished, young omnivore on standard doses (the cognitive benefits are real but depend heavily on baseline state; the evidence in this population is inconsistent and effect sizes are small)
- Trusting creatine monohydrate alternatives on marketing claims alone (creatine HCl, Kre-Alkalyn, creatine ethyl ester, and similar marketed variants have not demonstrated superior efficacy in head-to-head trials; monohydrate remains the evidence-backed standard)
Mechanisms Of Action
Simple:
- Creatine acts as an energy reserve that can instantly regenerate ATP when demand spikes, acting as a phosphate donor via the creatine kinase reaction.
- When muscle or brain cells run out of readily available ATP, phosphocreatine donates a phosphate group to ADP in milliseconds, restoring ATP, buying time for mitochondria to ramp up.
- The brain is the most energetically demanding organ in the body. More available phosphocreatine means more ATP reserve during high cognitive demand, sleep deprivation, or neurological stress.
- Low creatine in the prefrontal cortex is associated with depression, and increasing it via supplementation appears to improve antidepressant response.
- In muscle, more phosphocreatine means more capacity for repeated maximal contractions before fatigue sets in.
Advanced:
- Creatine kinase system and spatial energy buffering: Creatine kinase (CK) isoforms are strategically positioned at sites of high ATP consumption (myofibrillar actomyosin ATPase, SR Ca2+-ATPase) and at mitochondria (MtCK). The PCr/Cr couple acts as an energy shuttle: MtCK at the inner mitochondrial membrane converts ATP to PCr and ships it to cytosolic sites of ATP demand, where cytosolic CK regenerates ATP from PCr. This spatial buffering allows rapid delivery of high-energy phosphate from the mitochondria to anywhere in the cell without relying on ATP diffusion. R
- Brain creatine and the blood-brain barrier: SLC6A8 is expressed on the luminal membrane of brain capillary endothelial cells (the BBB) and is the only demonstrated route by which creatine enters the CNS from the periphery. Most neurons express AGAT and GAMT and can synthesize creatine locally from guanidinoacetate transported by SLC6A8. This means brain creatine comes from two sources: peripheral dietary/supplemental creatine crossing the BBB via SLC6A8, and local synthesis within CNS cells. This dual supply is why SLC6A8 deficiency causes brain creatine depletion even though the synthesis enzymes are present. R
- Neuroprotective mechanisms: Creatine reduces mitochondrial permeability transition (the opening of the mitochondrial permeability transition pore that triggers apoptosis) by stabilizing the inner mitochondrial membrane. It also directly scavenges reactive oxygen species (direct antioxidant activity) and reduces glutamate-induced excitotoxicity by maintaining cellular energy status, which limits pathological NMDA receptor activation that requires ATP depletion to occur maximally. R
- Antidepressant mechanism: Depression is associated with mitochondrial dysfunction and impaired brain bioenergetics in the prefrontal cortex and limbic structures. Creatine increases PCr/ATP ratio in these regions, restoring cellular energy homeostasis. It also modulates the dopaminergic system: creatine administration upregulates dopamine receptor expression and enhances dopamine transporter activity in the prefrontal cortex. Separately, creatine's methylation of GAA (via GAMT using SAM-e) competes for the methyl donor SAM-e, meaning high GAA accumulation (as in GAMT deficiency) depletes SAM-e and impairs methylation broadly. Normalizing creatine synthesis relieves this SAM-e competition, which may have secondary effects on mood through improved methylation capacity. R
- Sleep deprivation reversal: Sleep deprivation reduces brain PCr and ATP concentrations in regions associated with complex cognitive function. A single high creatine dose (0.35g/kg) compensates for this by providing an immediate exogenous source of phosphate buffer. In sleep-deprived subjects, creatine increased cerebral ATP-beta in regions with low baseline ATP-beta/PCr and decreased PCr/ATP where it was elevated, normalizing the energy distribution across brain regions. The net effect was measurable improvement in complex cognitive tasks that are otherwise degraded by sleep deprivation. R
- GAMT synthesis and SAM-e competition: The GAMT reaction that converts guanidinoacetate to creatine uses SAM-e as the methyl donor. GAMT is actually one of the highest-SAM-e-consuming reactions in the human body, consuming approximately 40-70% of all methylation in some tissues. In states of high creatine demand (low dietary intake, high synthesis requirement), this can create meaningful competition for SAM-e, potentially affecting other methylation-dependent pathways including methylation of DNA, histones, neurotransmitters, and myelin. Supplementing dietary creatine reduces the endogenous synthesis burden and may spare SAM-e for other methylation reactions. R
Genetics
AGAT (GATM Gene)
AGAT (L-arginine:glycine amidinotransferase) is encoded by the GATM gene on chromosome 15q21.
AGAT catalyzes the first and rate-limiting step of creatine synthesis in the kidney.
Severe biallelic loss-of-function variants cause AGAT deficiency (CDS type 1), presenting in infancy with global developmental delay, intellectual disability, hypotonia, and absent or delayed speech.
Unlike GAMT deficiency, GAA does not accumulate and the transporter is intact, so oral creatine supplementation is dramatically effective and early treatment can normalize development. R
More than 40 GATM variants have been identified.
Separately: A common AGAT polymorphism (rs16851622) has been studied for associations with muscle creatine storage efficiency and exercise response. Individuals with certain AGAT variants may have altered baseline creatine synthesis, potentially affecting responsiveness to supplementation.
GAMT (GAMT Gene)
GAMT encodes guanidinoacetate methyltransferase on chromosome 19p13.3.
GAMT catalyzes the second step of creatine synthesis, converting guanidinoacetate to creatine using SAM-e as the methyl donor.
Biallelic loss-of-function variants cause GAMT deficiency (CDS type 2), the most complex creatine deficiency syndrome due to both creatine depletion and guanidinoacetate neurotoxicity (GAA is directly toxic to the brain). R
More than 50 pathogenic variants have been identified, the most common being c.327G>A (p.K109K, a splice site variant) and c.59G>C (p.W20S). R
GAMT also consumes SAM-e at high rates, meaning GAMT variants that reduce creatine synthesis may paradoxically improve methylation efficiency by reducing SAM-e competition.
SLC6A8 (Creatine Transporter, X-Linked)
SLC6A8 encodes the creatine transporter (CrT/CT1) at chromosome Xq28.
This is the only transporter known to move creatine across the blood-brain barrier and into CNS cells. R
Loss-of-function mutations cause creatine transporter deficiency (CTD), the second largest cause of X-linked intellectual disability after Fragile X syndrome. R
Males are fully affected (hemizygous); females are variably affected (heterozygous) ranging from asymptomatic to learning disabilities and seizures. R
Critically, oral creatine supplementation does not work for CTD because the transporter is broken. R
Research into alternatives including creatine precursors, creatine esters that bypass SLC6A8, and gene therapy is ongoing.
More than 80 pathogenic SLC6A8 variants have been identified. R
Clinical Implication Of Creatine Genetics
Any patient with unexplained intellectual disability, speech delay, seizures, behavioral abnormalities, or autism-spectrum features should be screened for creatine deficiency syndromes with urine creatine/creatinine and guanidinoacetate measurements. R
AGAT and GAMT deficiency are fully treatable with creatine if caught early and can prevent or reverse intellectual disability.
CTD is currently not treatable with standard supplementation.
For the general population without diagnosed CDDs, common variants in GATM and GAMT may influence baseline creatine synthesis efficiency and responsiveness to supplementation, though the clinical effect size of these variants in neurotypical individuals is smaller than in deficiency states.
More Research
- Creatine monohydrate is the most studied ergogenic supplement in history, with over 500 peer-reviewed studies published. R
- A single high creatine dose (0.35g/kg) during sleep deprivation measurably changed brain high-energy phosphate ratios and improved cognitive performance on complex tasks, demonstrating acute central effects beyond the traditional chronic loading model. R
- Brain creatine increases with supplementation are dose-dependent and take longer to plateau than muscle creatine, suggesting that the 5g/day standard dose used in athletic contexts may underperform for cognitive endpoints. Doses of 10g/day or higher with sustained use are better supported for brain-specific goals. R
- GAMT, the second enzyme in creatine synthesis, is one of the body's largest consumers of SAM-e methyl groups. Supplementing dietary creatine reduces endogenous GAMT activity and may spare SAM-e for other methylation reactions, including those relevant to neurotransmitter synthesis, DNA methylation, and MTHFR-related methylation pathways. R
- For testing relevant to creatine metabolism, urine guanidinoacetate and creatine/creatinine ratios are the primary biomarkers for diagnosing creatine deficiency syndromes and are available through the Organic Acids Test (OAT) from Mosaic Diagnostics.
- Older adults with low creatine intake (less than 0.95g/day) show poorer cognitive function than those consuming more, independent of supplementation, supporting the view that the population-level cognitive benefits of animal protein consumption may partly reflect creatine content. R
- Preliminary CABA (Creatine to Augment Bioenergetics in Alzheimer's) trial data from the University of Kansas suggests creatine supplementation may have cognitive benefit in Alzheimer's disease by addressing the defective brain energy metabolism that is a hallmark of the condition. Larger trials are warranted. R
- SLC6A8 deficiency (creatine transporter deficiency) is the second largest cause of X-linked intellectual disability after Fragile X syndrome and is substantially underdiagnosed. It is not treatable with standard oral creatine, making diagnosis and genetic counseling particularly important for affected families. R
- Vegetarians typically respond most dramatically to creatine supplementation in both cognitive and physical domains due to their lower baseline tissue creatine stores from absence of dietary intake. R
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Lion's Mane
1000mg/day
Omega-3 (DHA)
2g/day
Phosphatidylserine
100mg 3x/day