GHK-Cu: The Copper Tripeptide That Resets Aging Gene Expression
By Jacob Gordon, INHC, FMT-CThree amino acids. One copper ion. A binding affinity tight enough that it effectively does not let go at physiological pH.
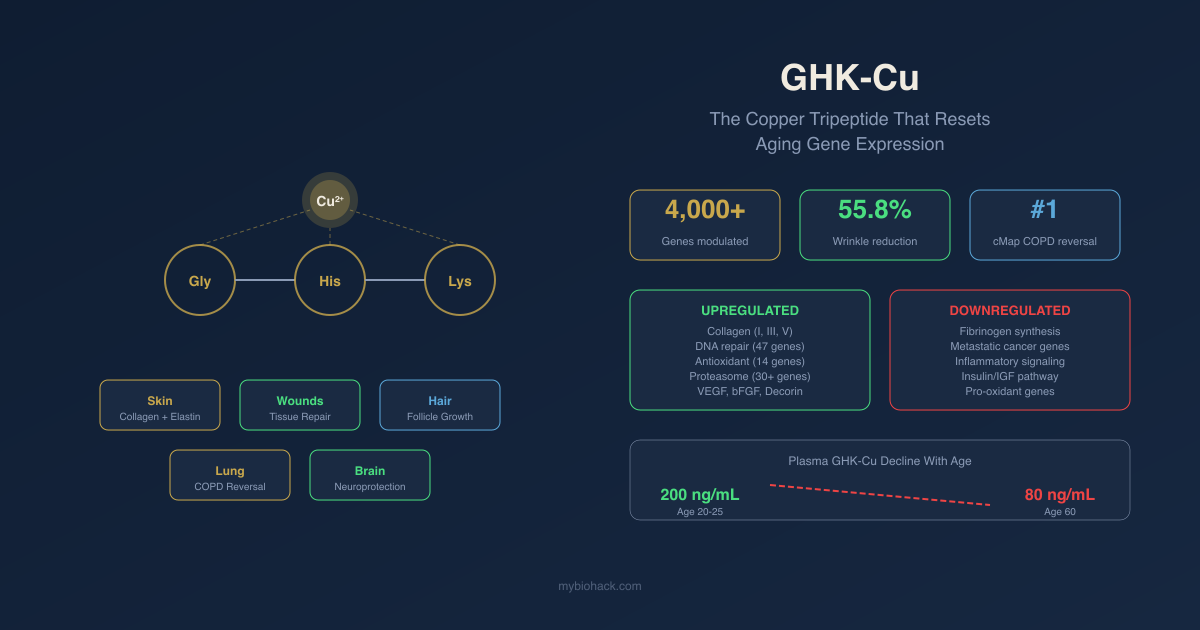
That is the whole molecule: glycine, histidine, lysine, chelated to copper(II) through three nitrogen atoms from histidine's imidazole ring, glycine's alpha-amino group, and the deprotonated amide bond between the first two residues. The resulting log K binding constant sits around 16.44, which means GHK-Cu is unusually stable as a copper complex under biological conditions. R
Loren Pickart discovered it in 1973 while studying why old human liver tissue would begin synthesizing proteins like younger tissue when exposed to a plasma fraction from young adults. Four years of work later, he isolated the active component. He spent the next 46 years building one of the most unusual bodies of work in peptide research before his death in 2023.
The unusual part: a molecule this simple modulates an estimated 4,000 human genes, placing it among the broadest genomic effectors of any naturally occurring peptide. The Broad Institute's Connectivity Map identified it as the top-ranked compound to reverse the gene expression signature of both emphysema-dominant COPD and metastatic colon cancer. R
This post covers the biology in depth.
What GHK-Cu Is And Where It Comes From
GHK stands for glycyl-L-histidyl-L-lysine, a tripeptide sequence found naturally in human plasma, saliva, and urine. Plasma levels average approximately 200 ng/mL in healthy adults aged 20 to 25. By age 60, circulating GHK has declined to roughly 80 ng/mL. The decline correlates with the well-documented age-related deterioration in wound healing capacity, collagen synthesis, and tissue repair. R
GHK is not thymus-specific, not organ-specific, and is not produced by a single dedicated gland. Instead, it is generated at the site of tissue injury. The tripeptide sequence Gly-His-Lys appears in the alpha-2(I) chain of type I collagen and in SPARC (secreted protein acidic and rich in cysteine), a matrix glycoprotein. When tissue proteases break down collagen and SPARC at injury sites, GHK is liberated, where it binds ambient copper ions and signals the repair cascade to begin. R
This gives GHK a built-in elegant logic: it is generated precisely when and where tissue damage occurs, in proportion to the amount of collagen being broken down. It then acts locally to recruit immune cells, stimulate fibroblasts, and initiate angiogenesis, before being cleared as the wound matures.
When SPARC later inhibits cell proliferation and new vessel growth, the repair cycle is naturally contained. R
The copper requirement:
GHK has high affinity for copper ions and circulates in plasma largely as the chelate GHK-Cu. Most researchers and most product formulations use GHK-Cu rather than GHK alone, though the two are difficult to completely distinguish biologically. Where the distinction matters, it is noted below.
Copper Ion: Why It Matters
Copper is an essential trace element and cofactor for several enzymes critical to connective tissue integrity and antioxidant defense.
Lysyl oxidase (LOX): The copper-dependent enzyme responsible for cross-linking collagen and elastin fibers into stable structures. Without adequate copper, collagen is synthesized but not properly cross-linked, producing structurally weaker connective tissue. GHK-Cu delivers copper directly to tissues where collagen synthesis is occurring, enabling proper LOX-mediated cross-linking. R
Lysyl hydroxylase: A copper-dependent enzyme that hydroxylates lysine residues in collagen, a modification required for both cross-linking and glycosylation. Proper hydroxylation is required for collagen's triple-helix stability and tissue-specific mechanical properties.
Superoxide dismutase (SOD): Copper-zinc SOD (CuZnSOD) is the primary cytoplasmic antioxidant enzyme. Copper delivery via GHK-Cu supports SOD activity. In wound and lung injury models, GHK-Cu treatment consistently increases SOD activity. R
Cytochrome c oxidase: The terminal enzyme in the mitochondrial electron transport chain is a copper-containing enzyme. Adequate copper delivery supports mitochondrial energy production in metabolically active healing tissue.
Antimicrobial properties: Copper ions have intrinsic broad-spectrum antimicrobial activity. In the wound environment, the copper component of GHK-Cu may contribute to reducing bacterial burden.
The concentration paradox:
GHK-Cu demonstrates a classic biphasic (hormetic) dose-response. At picomolar to low nanomolar concentrations, it is stimulatory. At higher concentrations, activity plateaus or reverses. In hair follicle studies, a 50 mg/mL concentration outperformed 100 mg/mL. This is consistent with how many cell-signaling molecules behave when they cross a concentration threshold that saturates or downregulates their receptor systems. Practically: more is not better with GHK-Cu. Standard research concentrations fall in the 1 to 100 nanomolar range for most biological effects. R
Genomic Mechanism: The 4,000-Gene Effect
The most striking feature of GHK-Cu research is what emerged when Pickart's team used the Broad Institute's Connectivity Map (cMap) to analyze its genomic fingerprint.
The Connectivity Map approach:
The cMap is a database of gene expression signatures for thousands of biological compounds, built from experiments in which human cell lines were exposed to each compound and gene expression changes were measured across the genome. When a disease condition produces a characteristic gene expression signature, the cMap can identify compounds whose signatures are the mathematical opposite, suggesting therapeutic potential.
GHK's cMap analysis revealed that it induces a 50% or greater change in expression in approximately 31.2% of all human genes tested. Among the 13,424 genes in the Broad Institute dataset at the time of analysis, GHK modulated over 4,000. R
The pattern of change:
The gene expression pattern GHK produces is not random amplification. It reverses the transcriptional signature of aging.
During human aging, inflammatory, cancer-promoting, and tissue-destructive genes trend upward. Regenerative, reparative, and cellular maintenance genes trend downward. GHK's genomic effect moves both categories in the opposite direction simultaneously. R
Key gene categories upregulated by GHK:
- Collagen synthesis genes (COL1A1, COL3A1, COL5A1)
- Elastin synthesis
- Decorin (a proteoglycan that organizes collagen fibers and prevents disordered scar formation)
- Angiogenesis factors: VEGF, bFGF (basic fibroblast growth factor), HGF
- DNA repair genes (47 upregulated, 5 downregulated in the analysis)
- Ubiquitin-proteasome system genes (>30 proteasome subunit genes upregulated by 60 to 90%)
- Antioxidant genes (14 stimulated, 2 pro-oxidant genes suppressed)
- TGF-beta pathway genes (critical for tissue remodeling and wound repair)
- Stem cell-related genes including p63 (epidermal stem cell marker) and various integrins R
Key gene categories downregulated by GHK:
- Fibrinogen synthesis genes (fibrinogen is a pro-inflammatory clotting factor and a strong predictor of cardiovascular mortality; GHK suppresses its synthesis)
- MMP-1 and MMP-2 at higher concentrations (though it also regulates their inhibitors TIMP-1/2 to achieve balanced remodeling)
- Genes driving metastatic cancer growth
- Insulin/insulin-like genes (suppressed in a pattern consistent with reduced anabolic signaling, potentially relevant to longevity biology) R
NF-kB modulation:
GHK's relationship with NF-kB is nuanced. It increases expression of the NF-kB2 gene by 103%, which looks pro-inflammatory. However, it simultaneously increases two NF-kB inhibitors: TLE1 by 762% and IL18BP (interleukin-18 binding protein, an endogenous IL-18 antagonist) by 295%. The net functional effect appears to be suppression of NF-kB activity despite the elevated NF-kB2 gene expression, because the inhibitors outweigh the activator. This is consistent with the anti-inflammatory effects observed in animal models. R
The proteasome system:
The ubiquitin-proteasome system (UPS) is the cell's primary protein quality control mechanism, degrading misfolded, damaged, or obsolete proteins. UPS activity declines with age, leading to accumulation of protein aggregates (a feature of Alzheimer's disease, Parkinson's disease, and general cellular senescence). GHK's strong upregulation of multiple proteasome subunit genes suggests it may support protein clearance and cellular housekeeping. This is a mechanistically plausible anti-aging effect that has not yet been directly confirmed in human clinical studies. R
Wound Healing And Tissue Repair
Wound healing is the best-characterized area of GHK-Cu biology and where the human data is most extensive.
Mechanism in wounds:
After tissue injury, collagen proteolysis releases GHK, which binds copper and becomes GHK-Cu. GHK-Cu then acts as a powerful chemoattractant for:
- Capillary endothelial cells (building new blood vessels via angiogenesis)
- Macrophages (clearing debris and secreting growth factors for wound contraction)
- Mast cells (releasing healing mediators) R
It stimulates fibroblast proliferation and activation, driving collagen type I (structural), type III (early-stage repair), and type V synthesis. Decorin is also upregulated, which organizes the resulting collagen fibers into ordered structures rather than disordered scar tissue. This decorin effect may be one reason GHK-Cu is associated with reduced scarring relative to normal wound healing. R
The MMP balance:
GHK-Cu modulates matrix metalloproteinases (MMPs) and their inhibitors (TIMPs) to achieve controlled tissue remodeling rather than either excessive breakdown or excessive fibrosis. At low concentrations (0.01 nM), it increases MMP1 and MMP2 gene expression alongside TIMP1. At higher concentrations, MMP expression is reduced. The practical result is a balanced ECM remodeling program that removes damaged tissue and rebuilds organized replacement matrix, rather than the runaway fibrosis seen in chronic wounds. R
Animal wound models:
In full-thickness rat wound models, GHK-Cu topically or intraperitoneally increased reepithelialization by 42% at day 4 and up to 61% at day 7 versus saline controls. Treated wounds contracted at least 11% more than controls by day 7. Increased collagen deposition and angiogenesis were observed histologically. R
In ischemic open wounds in rats (a clinically relevant model for diabetic ulcers and pressure wounds), GHK-Cu accelerated healing, reduced MMP-2 and MMP-9 concentrations, and lowered TNF-beta (a major inflammatory cytokine) compared with vehicle alone. R
In collagen dressing models incorporating GHK (peptide-incorporated collagen or PIC dressings), collagen synthesis increased 9-fold versus control wounds in healthy rats. Glutathione levels, ascorbic acid levels, epithelialization, and fibroblast and mast cell activation were all improved. R
Chronic wound limitation:
One documented practical issue is GHK-Cu's sensitivity to carboxypeptidase enzymes. The "wound serum" that develops on chronic wounds (diabetic ulcers, pressure wounds, venous stasis ulcers) contains carboxypeptidases from airborne bacteria, which rapidly break down GHK and likely other growth factors such as TGF-beta and PDGF. This may limit the efficacy of topical GHK-Cu application on infected or chronic wounds, favoring injectable or systemic delivery routes in these settings. R
Tissues beyond skin:
GHK-Cu has demonstrated wound healing activity across multiple tissue types:
- Gastrointestinal tract (stomach and intestinal lining repair)
- Bone (stimulates osteoblast spreading, attachment, and phenotype; used in collagen-graft scaffolds for bone defects)
- Liver (hepatoprotective; restores protein synthesis in aged liver tissue, the original discovery that led Pickart to GHK)
- Foot pads in dogs (an early veterinary application confirming practical wound healing utility)
- ACL repair in rat models (transient improvement in healing outcomes)
- Ligament tissue R
Skin: Collagen, Elastin, And Remodeling
Skin is the most thoroughly studied tissue application of GHK-Cu, both in preclinical models and human cosmetic trials.
Collagen and elastin:
GHK-Cu at 0.01 nM, 1 nM, and 100 nM concentrations increases collagen and elastin production in human adult dermal fibroblasts. It stimulates collagen types I, III, and V. It also increases dermatan sulfate, chondroitin sulfate, and decorin, the small proteoglycan that controls collagen fibril assembly and prevents disordered collagen deposition. R
The copper component drives proper collagen architecture through lysyl oxidase and lysyl hydroxylase activation, ensuring synthesized collagen forms structurally strong cross-linked fibers rather than disorganized matrix.
Fibroblast replicative vitality:
One of the earlier findings about GHK is its ability to restore replicative vitality to fibroblasts after radiation therapy. Irradiated human dermal fibroblasts treated with GHK-Cu at 1 nM showed increased expression of bFGF (basic fibroblast growth factor) and VEGF, both of which drive new blood vessel formation and support the vascular supply that irradiated tissues characteristically lose. R
Skin stem cells:
GHK upregulates p63, a transcription factor that marks epidermal stem cells and controls their proliferation and differentiation. It also upregulates multiple integrin family members (integrin alpha-3, integrin beta-1) that are critical for keratinocyte adhesion to the basement membrane and stem cell niche maintenance. R This stem cell support may underlie GHK-Cu's ability to restore the capacity of aged or damaged skin to regenerate.
Clinical cosmetic trials:
A randomized, double-blind trial in female volunteers compared GHK-Cu encapsulated in nano-lipid carrier twice daily for 8 weeks against a carrier-alone control and the commercially available peptide Matrixyl 3000. Compared to Matrixyl 3000, GHK-Cu produced a 31.6% reduction in wrinkle volume. Compared to carrier control, GHK-Cu reduced wrinkle volume by 55.8% and wrinkle depth by 32.8%. R
A 2024 meta-analysis of 5 randomized controlled trials (n = 289) for photoaging reported a standardized mean difference of -0.68 for fine lines (95% CI -1.02 to -0.34), indicating moderate evidence for efficacy. The limitations of this evidence base are real: small sample sizes and industry funding in a substantial proportion of trials. R
Photodamage and hyperpigmentation:
GHK-Cu reduces photodamage, improves skin clarity, reduces hyperpigmentation, and improves the dermal structure. It can penetrate the stratum corneum and act at the dermal level (assisted by formulation technologies), making it more than a surface cosmetic ingredient. R
Hair Follicle Biology
Why GHK-Cu affects hair:
Hair follicles are among the most metabolically active and regeneration-dependent structures in the body. They require coordinated fibroblast activity, angiogenesis, ECM remodeling, and controlled inflammation to cycle through anagen (growth), catagen (regression), and telogen (rest) phases. These are precisely the processes GHK-Cu regulates. R
Mechanisms in hair follicles:
GHK-Cu acts on hair follicles through several converging pathways:
Dermal papilla cells (the fibroblast-like cells at the base of each follicle that signal the follicle to grow) show stimulated proliferation and reduced apoptosis after GHK-Cu exposure. In 2007 dermal papilla cell studies, copper peptides reduced caspase-3 (the key apoptosis executioner enzyme) by 42.7% and shifted the Bcl-2/Bax survival balance toward cell protection. R
TGF-beta1 suppression: TGF-beta1 is a key signal that drives hair follicles prematurely into the catagen (regression) phase. GHK-Cu downregulates TGF-beta1, potentially extending the anagen growth phase. R
Wnt/beta-catenin activation: Wnt signaling is required for hair follicle morphogenesis, cycling, and stem cell activation. GHK-Cu upregulates beta-catenin, the key intracellular effector of Wnt signaling. In ex vivo follicle studies, GHK-Cu increased beta-catenin by 40%, comparable to valproic acid (a known Wnt activator). R
Stem cell activation: GHK-Cu's p63 and integrin upregulation in the follicle stem cell niche supports follicle regeneration. It increases hair follicle size (the key structural parameter that determines hair shaft diameter) and strengthens the dermal papilla against the miniaturization that drives androgenetic alopecia. R
VEGF and HGF stimulation: Vascular endothelial growth factor and hepatocyte growth factor produced in follicle vasculature drive hair growth in vitro and in vivo. GHK-Cu increases both, providing the blood supply and paracrine growth factor signaling that active follicles require. R
Clinical evidence for hair:
A 2021 Phase II randomized controlled trial in 45 males with androgenetic alopecia applied a 0.5% GHK-Cu lotion. 72% of subjects reported greater than 20% hair density increase at 6 months by phototrichogram (p = 0.002 vs placebo). R
A 2016 randomized double-blind placebo-controlled trial used the compound ALAVAX, which combines GHK peptide with 5-aminolevulinic acid (5-ALA, a mitochondrial energy precursor). Treatment produced 52 to 72 additional hairs per cm2 versus 9.6 in the placebo group, with zero side effects. The lower dose (50 mg/mL) outperformed the higher dose (100 mg/mL), consistent with GHK-Cu's hormetic dose-response. R
Comparison to minoxidil:
GHK-Cu and minoxidil work through different mechanisms. Minoxidil is a vasodilator that extends the anagen phase by improving scalp blood flow. GHK-Cu works through regenerative pathways: fibroblast and stem cell activation, TGF-beta1 suppression, ECM remodeling, and angiogenesis via VEGF. The mechanisms are complementary, which is why GHK-Cu plus minoxidil combination approaches show synergistic signals. R
GHK-Cu does not affect hormones or DHT. It is non-hormonal and carries none of finasteride's endocrine risk.
The honest limitation:
GHK-Cu can only support follicles that are still biologically active. Once a follicle has fully miniaturized and become fibrotic, no topical or systemic agent yet proven in clinical trials reliably restores it. Catching hair thinning early, when follicles are miniaturizing but not yet destroyed, is when GHK-Cu has the most potential impact.
Delivery challenge:
Standard topical application of GHK-Cu in aqueous solution leaves much of the peptide outside the stratum corneum. A 2024 study developed an ionic liquid-based microemulsion (IL-M) system that improved local copper peptide delivery approximately 3-fold while retaining biological function. In mice, the IL-M formulation produced earlier anagen phase entry than either standard GHK-Cu topical or minoxidil. R
Lung And COPD
The COPD application is the most scientifically rigorous demonstration of GHK-Cu's gene-resetting capability and is the study Pickart considered the strongest evidence of GHK's biological relevance.
The COPD gene signature:
A collaborative study across Boston University, University of Groningen, University of British Columbia, and University of Pennsylvania identified 127 genes whose expression levels were significantly associated with regional emphysema severity in COPD patient lung tissue. Genes involved in inflammation were upregulated; genes involved in tissue remodeling and repair, including key TGF-beta pathway genes, were downregulated. More severe emphysema correlated directly with the degree of gene expression change. R
Connectivity Map prediction:
The researchers ran this 127-gene signature through the Broad Institute's Connectivity Map. Of 1,309 biologically active molecules in the database, GHK ranked first as the compound most predicted to reverse the emphysema gene expression signature. R
In vitro confirmation:
Lung fibroblasts from the diseased regions of COPD patients have a specific defect: they cannot contract and remodel collagen gel, a functional marker of normal fibroblast competence. When these fibroblasts were treated with GHK at 10 nM, they restored normal collagen contraction and remodeling. They also elevated integrin beta-1 expression and reorganized their actin cytoskeleton. The same restoration occurred when fibroblasts were treated with TGF-beta itself, confirming GHK was recapitulating TGF-beta pathway activity. R
Acute lung injury:
In LPS-induced acute lung injury mouse models, GHK-Cu:
- Attenuated histological lung damage
- Suppressed inflammatory cell infiltration into the lung parenchyma
- Increased SOD activity (antioxidant defense)
- Decreased TNF-alpha and IL-6 production
- Blocked phosphorylation of NF-kB p65 and p38 MAPK in lung cells R
The suppression of NF-kB p65 phosphorylation and p38 MAPK is mechanistically consistent with the genomic NF-kB inhibition data (via TLE1 and IL18BP upregulation) discussed in the genomics section.
GHK has not yet entered clinical trials for COPD. The animal and genomic data are compelling, but no human COPD trial has been conducted. R
Anti-Inflammatory And Antioxidant Mechanisms
Cytokine modulation:
GHK-Cu consistently reduces pro-inflammatory cytokines across multiple models and tissues. In ischemic wounds, it lowered TNF-beta compared to vehicle controls. In LPS-induced lung injury, it reduced TNF-alpha and IL-6. R In human fibroblast cultures, GHK-Cu decreased TGF-beta1 (acting pro-inflammatory/pro-fibrotic in this context) while maintaining the tissue-remodeling TGF-beta signaling required for repair. R
NF-kB suppression without blanket suppression:
The mechanism by which GHK modulates NF-kB is indirect and nuanced, as described in the genomics section. Rather than directly blocking NF-kB like a pharmaceutical antagonist, GHK upregulates NF-kB's endogenous inhibitors (TLE1 and IL18BP), which tip the balance toward reduced NF-kB activity while preserving the receptor infrastructure. This likely explains why GHK-Cu does not suppress immunity broadly the way corticosteroids do, while still demonstrating meaningful anti-inflammatory effects. R
p38 MAPK:
p38 MAPK is activated by cellular stress signals (cytokines, UV radiation, heat, osmotic shock) and drives inflammation, differentiation, apoptosis, and autophagy. GHK-Cu blocks p38 MAPK phosphorylation, reducing the downstream inflammatory gene program that p38 activates. R
Antioxidant enzyme support:
GHK-Cu increases SOD activity across multiple models. It protects keratinocytes from UVB radiation, blocks hepatic damage from dichloromethane radicals, blocks reactive oxygen species (ROS) production, and detoxifies lipid peroxidation products including acrolein (a toxic aldehyde produced by oxidative stress). R
The genomic data shows GHK upregulates 14 antioxidant genes while suppressing 2 pro-oxidant genes, with the antioxidant-to-pro-oxidant ratio strongly favoring a net protective effect.
Cancer Biology
GHK-Cu's cancer biology is complex. The Connectivity Map placed it first to reverse the gene expression signature of metastatic colon cancer, which initiated a series of in vitro experiments.
Apoptosis reactivation:
When three lines of human cancer cells (SH-SY5Y neuroblastoma, U937 histolytic lymphoma, and a breast cancer line) were incubated with GHK at 1 to 10 nM, the programmed cell death system (apoptosis) was reactivated and cell growth was inhibited. R
In sarcoma cells in mice, GHK similarly inhibited growth and changed the gene expression of over 80 genes in an anti-growth pattern. R
Colon cancer gene expression:
GHK suppressed 70% of genes overexpressed in an aggressive, metastatic form of colon cancer. The suppressed genes included "node molecules" (YWHAB, MAP3K5, LMNA, APP, GNAQ, F3, NFATC2, and TGM2) involved in regulating multiple biological functions through complex networks. R
The counterpoint:
GHK's pro-growth effects on fibroblasts, endothelial cells, and mesenchymal cells that are beneficial in wound healing and tissue repair share mechanistic overlap with processes tumors exploit for their own growth and angiogenesis. The picture is not uniformly anti-cancer. GHK's effects in cancer appear highly context- and cell-type-dependent. In cells where the apoptotic program is already disrupted (cancer cells), GHK appears to restore it. In normal tissue, GHK supports growth and repair. Whether this selectivity would hold in the complex tumor microenvironment is unknown. R
The cancer data is entirely preclinical. No human cancer trials of GHK-Cu have been conducted. Given its generally low toxicity and widespread cosmetic use, this is an area Pickart considered a major priority for future clinical investigation.
Nervous System And Cognitive Aging
Nerve outgrowth:
Multiple in vitro studies found that GHK stimulates the outgrowth of cultured neurons. In nerve regeneration models, collagen tubes impregnated with GHK (without copper) placed at nerve stumps showed:
- Increased production of nerve growth factor (NGF)
- Increased NT-3 and NT-4 (neurotrophin-3 and neurotrophin-4/5)
- Increased migration of cells into the collagen tube
- Faster regeneration of nerve fibers R
BDNF and neuroprotection:
GHK increases production of neurotrophic factors. BDNF (brain-derived neurotrophic factor) is among the growth factors elevated, and BDNF is well established as a protective factor against neurodegeneration. GHK-Cu also supports angiogenesis into damaged neural tissue, relevant because the brain is highly metabolically active and vulnerable to vascular insufficiency. R
Cognitive aging:
In aging mice, GHK partially reversed cognitive impairment by targeting anti-inflammatory and epigenetic pathways. The Connectivity Map analysis identified that GHK's gene expression effects include regulation of nervous system physiology, development, and maintenance genes, with relevance to Alzheimer's disease and Parkinson's disease pathways. R
The proteasome upregulation discussed earlier is relevant here: protein aggregate clearance via the UPS is impaired in both Alzheimer's and Parkinson's disease, and GHK's strong induction of proteasome genes positions it as a theoretically relevant candidate.
Anti-anxiety and anti-pain:
GHK has a physical structure similar to cimetidine (an H2 receptor blocker also used for pain reduction in some contexts). In mouse hot-plate pain assays, GHK reduced pain at 0.5 mg/kg. Anti-anxiety (anxiolytic) and anti-aggression effects have also been documented in animal models. R
These are animal data only; no human anxiety, pain, or cognitive trials of GHK-Cu have been completed.
Other Tissues And Systemic Effects
Bone:
GHK-Cu promotes osteoblast cell spreading, attachment, and phenotype expression. In collagen-graft scaffolds supplemented with GHK, bone healing and bone morphological features improved compared with scaffold alone. GHK also stimulates chondroitin sulfate synthesis, relevant to cartilage matrix integrity. R
Liver:
The 1973 discovery was hepatic: a plasma fraction from young humans caused aged liver tissue to synthesize proteins at youthful rates. That fraction contained GHK. GHK remains hepatoprotective in subsequent models, with documented protection against chemical hepatic damage. R
Cardiovascular:
GHK suppresses fibrinogen synthesis. Fibrinogen is both a coagulation factor and one of the strongest predictors of cardiovascular mortality (elevated fibrinogen predicts heart attack and stroke risk independently of other risk factors). Whether GHK-Cu's fibrinogen-suppressing genomic effect translates to meaningful reduction in serum fibrinogen in humans has not been studied. R
GHK-Cu also promotes angiogenesis, improves blood flow into damaged tissues, and has anti-coagulant properties in the wound environment. R
Stem cells:
GHK increases cellular stemness and stimulates trophic factor secretion from mesenchymal stem cells. It upregulates epidermal stem cell markers (p63) and integrins required for stem cell niche maintenance. This stem cell-supporting property, combined with growth factor induction (VEGF, bFGF, HGF), positions GHK-Cu as a potential systemic regenerative support molecule. R
Clinical Evidence And Trials
Topical skin (best evidence):
The 8-week randomized controlled cosmetic trial (GHK-Cu encapsulated in nano-lipid carrier) is the strongest controlled human data: 55.8% wrinkle volume reduction versus control, 32.8% wrinkle depth reduction. Meta-analysis of 5 RCTs for photoaging (n = 289) shows SMD -0.68 for fine lines. Multiple additional smaller double-blind trials confirm improvements in skin elasticity, firmness, and thickness at 8 to 12 weeks. Limitations: small samples, industry funding in a substantial proportion of studies. R
Hair follicle (moderate evidence):
The 2021 Phase II RCT (n = 45, androgenetic alopecia males, 6 months, 0.5% topical GHK-Cu) with 72% response rate is the strongest controlled hair data. The 2016 double-blind RCT using GHK + 5-ALA compound (ALAVAX) showing 52 to 72 extra hairs per cm2 provides additional controlled evidence. Total controlled hair trials remain small; larger, longer trials are needed before drawing definitive conclusions. R
Wound healing (strong preclinical, limited clinical):
Animal wound data across multiple labs, tissue types, and wound models is among the most replicated in this field. Phase II surgical scar data (n = 40) showing 35% scar volume reduction versus silicone at 3 months is encouraging but requires replication. The carboxypeptidase degradation issue in chronic wounds complicates topical trial design.
COPD, cancer, neurology (preclinical only):
No completed human clinical trials exist for these applications despite compelling genomic and animal data. Clinical trials for COPD were proposed by Pickart's team and identified as a priority; none have launched as of early 2026.
Safety:
Topical GHK-Cu has decades of cosmetic use history without documented serious adverse events. Pooled data from 12 studies (n = 892) reports mild erythema in 4.2% and pruritus in 2.1% of users, with no systemic copper overload (serum copper levels unchanged with topical application). Injectable safety data is limited compared to topical. No hepatotoxicity or significant allergic reactions have been documented. R
Administration, Dosing, And Regulatory Status
Regulatory status (important):
GHK-Cu has no FDA-approved indications for any medical condition. Topically in cosmetic products, it is regulated as a cosmetic ingredient (21 CFR 700), not a drug. This means manufacturers cannot make disease treatment or prevention claims.
Injectable GHK-Cu was placed in the FDA's Category 2 (prohibited from commercial compounding under 503B) as of 2023 to 2024. Category 2 designation generally means the FDA has determined there are insufficient data to support compounding for broader use. Some 503A compounding pharmacies (which compound for individual patients with a specific prescription) continue to offer GHK-Cu preparations, including scalp solutions and injectable forms, in jurisdictions where this remains permissible. The regulatory landscape for compounded peptides is actively evolving.
Topical:
For skin anti-aging: 0.1 to 0.5% concentration in a stable carrier formulation, applied twice daily. Clinical trials measured outcomes at 8 to 12 weeks; meaningful changes in deeper parameters (collagen density, skin thickness by ultrasound) typically require 2 to 3 months.
For scalp/hair: 0.5% solution applied once to twice daily to affected scalp regions. Treatment courses of 3 to 6 months are standard. Formulation matters enormously: standard aqueous GHK-Cu has poor stratum corneum penetration; liposomal, nano-lipid carrier, or ionic liquid microemulsion formulations significantly improve delivery.
Topical GHK-Cu is widely available in cosmetic serums, creams, and dedicated scalp products without a prescription.
Injectable (where available):
No standardized dosing protocol exists for injectable GHK-Cu. Clinical investigators have used doses in the range of 0.5 to 5 mg per session, though this is extrapolated from preclinical effective concentrations rather than from completed human dose-finding trials. Subcutaneous and intramuscular routes have been used. The very short plasma half-life of the peptide (minutes) limits systemic effects from single injections; regular dosing schedules are used in clinical settings.
The concentration hormesis caveat:
GHK-Cu is not a case where more produces better effects. The dose-response curve is distinctly non-linear. Optimal activity is typically in the low nanomolar range in cell culture; in topical formulations, the 0.5 to 1% concentration range appears to be the practical sweet spot in the few controlled trials that have tested multiple concentrations. Higher concentrations can produce reduced or reversed effects on cell proliferation and follicle stimulation.
Stability:
GHK-Cu is sensitive to carboxypeptidase degradation in infected wound environments. It is also sensitive to pH extremes and strong oxidizing conditions. Stable cosmetic formulations use encapsulation technologies (liposomes, nano-lipid carriers, cyclodextrins) to protect the peptide. Refrigerated storage is recommended for injectable preparations.
Mechanisms Of Action
Simple:
- GHK-Cu is a tripeptide (glycine-histidine-lysine) bound to copper(II) that is naturally generated at wound sites when tissue proteases break down collagen and SPARC.
- Plasma levels peak around 200 ng/mL at age 20 and decline to 80 ng/mL by age 60, correlating with declining tissue repair capacity.
- It works by modulating gene expression across approximately 4,000 human genes, shifting the pattern from an aging (inflammatory/destructive) profile toward a regenerative (repair/protective) profile.
- In wounds, it attracts immune cells, endothelial cells, and fibroblasts; stimulates collagen types I, III, and V; organizes collagen fibers via decorin; drives angiogenesis via VEGF and bFGF; and balances MMP-TIMP activity for controlled tissue remodeling.
- On skin, it increases collagen, elastin, and glycosaminoglycans while reducing wrinkle depth; on hair follicles, it extends the growth phase by suppressing TGF-beta1 and activating Wnt/beta-catenin signaling.
- In the lung, Connectivity Map analysis identified it as the top compound to reverse the emphysema gene signature in COPD; in vitro, it restored COPD fibroblast function via TGF-beta pathway activation.
- Its anti-inflammatory mechanism is indirect: it upregulates NF-kB's endogenous inhibitors (TLE1 and IL18BP) rather than directly blocking the receptor.
- Copper delivery via GHK-Cu activates lysyl oxidase (collagen cross-linking), superoxide dismutase (antioxidant defense), and cytochrome c oxidase (mitochondrial energy).
- It has no FDA-approved medical indications; injectable forms are prohibited from commercial compounding in the US; topical cosmetic use has decades of safety history.
Advanced:
- Copper chelation chemistry and biological targeting: GHK coordinates Cu(II) through a square-planar arrangement involving three nitrogen donors: the imidazole nitrogen of histidine (the strongest copper-binding nitrogen in biomolecules), the alpha-amino nitrogen of glycine, and the deprotonated amide nitrogen between glycine and histidine. The log K binding constant of approximately 16.44 at physiological pH is high for a tripeptide, providing thermodynamic stability that allows GHK-Cu to survive plasma half-life long enough to reach target tissues while being labile enough to donate copper to copper-requiring enzymes. The histidine imidazole's unusually high copper affinity among common amino acids is the structural reason a tripeptide can achieve this stability. When GHK-Cu encounters lysyl oxidase at the cell surface, it donates copper to the enzyme's active site, activating LOX-mediated crosslinking without requiring systemic copper supplementation. R
- SPARC-liberated GHK as a damage-sensing alarm system: SPARC (secreted protein acidic and rich in cysteine, also called osteonectin or BM-40) is an ECM glycoprotein that contains the GHK sequence in its functional copper-binding domain. SPARC has a dual role: it promotes cell proliferation and angiogenesis when cleaved, releasing GHK; and in its intact form, SPARC inhibits cell proliferation and angiogenesis, terminating the repair signal. This creates an elegant negative feedback loop: more tissue damage means more collagen and SPARC proteolysis, more GHK-Cu generation, and more repair signaling. As the tissue heals and matrix is rebuilt, less SPARC is being cleaved, GHK levels fall, and intact SPARC inhibits the vascular and proliferative response. R
- TGF-beta pathway paradox: GHK-Cu simultaneously downregulates TGF-beta1 (where TGF-beta1 is acting in its pro-inflammatory/pro-fibrotic role, such as driving premature catagen in hair follicles or driving fibrosis in chronic wounds) and upregulates TGF-beta pathway genes (where TGF-beta is acting in its wound repair/collagen synthesis role, as in the COPD fibroblast rescue). This selectivity is possible because TGF-beta operates through different receptor complexes and intracellular mediators (SMAD2/3 for fibrotic signaling versus SMAD1/5/8 via ALK1 for wound repair signaling) and different cell types respond differently to the same TGF-beta ligand concentration. GHK appears to restore the tissue-repair arm of TGF-beta signaling while suppressing the fibrotic/inflammatory arm, a distinction that has major implications for its utility in chronic inflammatory and fibrotic conditions.
- Decorin and the anti-fibrotic mechanism: Decorin is a small leucine-rich proteoglycan that decorates collagen fibrils (hence its name) and performs several critical functions: it controls collagen fibril diameter and assembly, it sequesters and inactivates TGF-beta (the primary driver of fibrosis), and it inhibits cell proliferation by binding to the EGF receptor. GHK-Cu's strong upregulation of decorin synthesis explains several apparently unrelated effects: reduced scarring (decorin prevents disordered collagen deposition), reduced fibrosis (decorin neutralizes fibrogenic TGF-beta), and reduced cell overgrowth in regenerating tissue (decorin's EGF receptor binding prevents excessive proliferation). The same molecule that builds more collagen also organizes it correctly and prevents too much of it from being made. R
Genetics
Collagen gene variants and GHK-Cu response:
COL1A1 and COL1A2 polymorphisms affect baseline collagen production and response to stimuli. The COL1A1 Sp1 binding site polymorphism (rs1800012) alters COL1A1 transcription factor binding and is associated with reduced collagen synthesis. Individuals with this variant may have blunted collagen synthesis responses to GHK-Cu stimulation, though this interaction has not been directly tested.
Lysyl oxidase (LOX) variants:
LOX is the copper-dependent enzyme that cross-links collagen and elastin, and it is GHK-Cu's primary collagen maturation target. Rare LOX loss-of-function mutations cause cutis laxa and arterial aneurysm (OMIM 219100). More common LOX variants affect connective tissue quality and wound healing. Since GHK-Cu delivers copper to activate LOX, the baseline LOX functional status would determine how much benefit copper delivery can provide. Low LOX activity (whether from genetic or zinc/copper deficiency) is the rate-limiting step GHK-Cu addresses.
MMP variants:
MMP1 and MMP3 promoter polymorphisms (particularly the MMP1 -1607 1G/2G variant) alter baseline matrix metalloproteinase activity. GHK-Cu modulates both MMP expression and TIMP expression to achieve balanced ECM remodeling. Higher baseline MMP activity (from permissive MMP promoter variants) combined with GHK-Cu might produce overly aggressive matrix remodeling, while lower baseline MMP activity might benefit more substantially from GHK-Cu's stimulation of remodeling.
VEGF variants:
VEGF promoter variants (particularly rs2010963, -634 G/C) affect baseline VEGF production. Since GHK-Cu's angiogenic effects are partly VEGF-mediated, individuals with constitutively lower VEGF expression (GG genotype) might show more substantial angiogenic responses to GHK-Cu than those with already-high VEGF expression.
SLC31A1 (copper transporter CTR1):
Copper import into cells depends on the high-affinity copper transporter SLC31A1 (CTR1). Variants affecting CTR1 expression or function would be expected to alter how effectively cells import and utilize copper delivered by GHK-Cu. Common SLC31A1 variants have been reported but not systematically studied in the context of GHK-Cu response.
More Research
- COPD clinical trials: The Connectivity Map COPD finding generated substantial scientific interest in clinical translation. No completed human COPD trial has emerged, despite the compelling genomic prediction and the in vitro confirmation in COPD patient cells. The likely pathway to a COPD trial would require an inhaled or nebulized GHK-Cu formulation with pharmacokinetic data showing adequate lung tissue distribution, followed by a Phase II proof-of-concept trial in emphysema-dominant COPD patients with measurable gene expression or pulmonary function outcomes. R
- Fibrinogen suppression and cardiovascular risk: GHK's documented suppression of fibrinogen synthesis genes is mechanistically interesting given fibrinogen's role as both a coagulation factor and an independent cardiovascular risk predictor (elevated fibrinogen predicts MI and stroke beyond LDL cholesterol and other standard risk factors). Whether systemic GHK-Cu administration translates to measurable serum fibrinogen reduction in humans would be a relatively straightforward trial to design and would address one of the most clinically actionable potential systemic benefits. R
- Proteasome activation and neurodegeneration: GHK's upregulation of more than 30 proteasome subunit genes is one of the more exciting but unconfirmed genomic predictions. Impaired proteasome activity is a consistent feature of aging neurons and of both Alzheimer's and Parkinson's disease pathology (where proteasomal failure allows tau, alpha-synuclein, and other aggregates to accumulate). An aging animal model study examining whether GHK-Cu supplementation maintains proteasome activity and reduces aggregate burden would be the appropriate next step before human cognitive trials.
- Delivery technology: The comparison between standard topical GHK-Cu and ionic liquid microemulsion formulations (3-fold improved delivery) suggests that formulation is a major driver of clinical outcome. Systematic head-to-head comparisons of delivery systems (liposomal, nanoparticle, microneedle, IL-M, dissolving microneedle patch) would clarify the optimal delivery approach for each application. The hair follicle application especially depends on stratum corneum penetration, and no standardized formulation exists.
- Oral bioavailability: GHK is present naturally in urine, suggesting some small amount survives digestion or is synthesized from dietary amino acids. Whether oral GHK-Cu supplementation could meaningfully elevate plasma GHK has not been rigorously tested. Given that plasma GHK peaks at 200 ng/mL in young adults (a detectable, physiologically relevant concentration), even partial oral bioavailability of a supplemental dose could have clinical significance. A pharmacokinetic study of oral GHK-Cu in humans comparing plasma levels to baseline would be straightforward and highly informative. R
- The regulatory path forward: GHK-Cu's FDA compounding prohibition for injectable forms reflects both the general tightening of peptide compounding regulation and the absence of IND (Investigational New Drug) applications for GHK-Cu in the US regulatory system. A research institution pursuing a clinical IND application for a specific indication (wound healing, COPD, or a dermatological application with a defined endpoint) would be the route to generating the human safety and efficacy data that might eventually support an NDA or a reversal of the compounding restriction. The extensive preclinical safety record is a meaningful asset in this regulatory pathway.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Quercetin
500mg 2x/day
SPM Active (Pro-resolving Mediators)
2 softgels/day
Curcumin (Liposomal)
500mg 2x/day