Vasopressin (ADH): The Hormone That Controls Your Water Balance, Blood Pressure, And Stress Response
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Arginine Vasopressin (AVP), also called Anti-Diuretic Hormone (ADH), is a nine amino acid peptide that determines how much water your kidneys retain, how much your blood vessels constrict, and how strongly your stress axis fires.
In this post, we will discuss what vasopressin is, how it works at the receptor level, what happens when it is too high or too low, which conditions overlap with vasopressin dysregulation, how to support healthy vasopressin signaling, what to avoid, relevant testing, mechanisms of action, genetics, and more research.

Basics Of Vasopressin
Arginine Vasopressin (AVP) is a peptide hormone synthesized in the magnocellular neurons of the supraoptic nucleus (SON) and paraventricular nucleus (PVN) of the hypothalamus. R
It is produced as a larger precursor called prepro-vasopressin, which is cleaved during axonal transport into AVP, neurophysin II (the carrier protein), and copeptin (a glycopeptide released in equimolar amounts that serves as a stable clinical biomarker). R
The mature peptide is stored in secretory vesicles in the posterior pituitary (neurohypophysis) and released into systemic circulation in response to specific physiological triggers. R
The half-life of AVP in plasma is only 10 to 35 minutes, which is why the body relies on moment-to-moment regulation rather than sustained baseline levels. R
The two most important triggers for AVP release are:
- Increased plasma osmolality (detected by hypothalamic osmoreceptors, which are the most sensitive regulators) R
- Decreased blood volume or blood pressure (detected by cardiopulmonary and arterial baroreceptors) R
Osmoreceptors respond to changes as small as 1 to 2% in plasma osmolality. R
Baroreceptor-driven release requires a larger stimulus (typically 5 to 10% drop in blood volume) but produces a much more aggressive AVP response and becomes the dominant control mechanism during hemorrhage or severe dehydration. R
Non-osmotic, non-hemodynamic triggers also stimulate AVP release: (not exclusive list)
- Angiotensin II R
- Nausea (one of the most potent non-osmotic triggers) R
- Nicotine R
- Pain R
- Stress and CRH activation R
AVP acts through three G-protein coupled receptors (GPCRs):
- V1a (vascular smooth muscle, liver, platelets) couples to Gq and triggers vasoconstriction via phospholipase C, IP3, and intracellular calcium release R
- V1b (V3) (anterior pituitary corticotrophs) couples to Gq and drives ACTH release, linking vasopressin directly to the HPA axis R
- V2 (renal collecting duct principal cells) couples to Gs and activates adenylyl cyclase, raising cAMP, which triggers aquaporin-2 (AQP2) water channel insertion into the apical membrane R
The V2 receptor is the one responsible for the "antidiuretic" effect: water reabsorption from the collecting duct lumen back into the bloodstream.
What Causes Vasopressin Dysregulation
Vasopressin can be dysregulated in both directions: too much (water retention, hyponatremia) or too little (polyuria, dehydration).
Causes Of Elevated Vasopressin (SIADH)
Syndrome of Inappropriate Antidiuretic Hormone (SIADH) occurs when AVP is secreted despite low plasma osmolality or adequate blood volume. R
The result is dilutional hyponatremia: excess water retention dilutes serum sodium below 135 mEq/L. R
Common causes of SIADH include: (not exclusive list)
- CNS disorders (meningitis, encephalitis, traumatic brain injury, subarachnoid hemorrhage) R
- Ectopic AVP secretion (small cell lung carcinoma is the classic example) R
- Medications (SSRIs, carbamazepine, cyclophosphamide, vincristine, oxytocin, desmopressin, amitriptyline, and NSAIDs) R
- Post-surgical states (pain and nausea are potent AVP triggers) R
- Pulmonary disease (pneumonia, tuberculosis, positive-pressure ventilation) R
Causes Of Low Vasopressin (Diabetes Insipidus)
Diabetes insipidus (DI) is characterized by the excretion of large volumes of dilute urine (up to 20 liters per day in severe cases) and intense thirst. R
There are two forms:
- Central DI (AVP Deficiency): the hypothalamus or pituitary fails to produce or release adequate AVP, caused by head trauma, pituitary surgery, autoimmune hypophysitis, granulomatous disease, or idiopathic destruction of magnocellular neurons R
- Nephrogenic DI (AVP Resistance): the kidney collecting duct does not respond to AVP, caused by lithium use (most common acquired cause), hypercalcemia, hypokalemia, tubulointerstitial disease, or genetic mutations in AVPR2 or AQP2 R
Both forms produce the same clinical picture (polyuria, polydipsia, risk of hypernatremia), but treatment differs entirely.
How The Kidney Uses Vasopressin
The kidney is where vasopressin does most of its physiological work.
AVP circulates in the blood and reaches the basolateral membrane of principal cells in the renal collecting duct. R
It binds the V2 receptor, which activates the Gs protein and stimulates adenylyl cyclase. R
This raises intracellular cyclic AMP (cAMP), which activates protein kinase A (PKA). R
PKA phosphorylates aquaporin-2 (AQP2) water channels stored in intracellular vesicles, triggering their fusion with the apical (luminal) membrane. R
Once AQP2 is inserted, water moves from the dilute tubular fluid in the lumen, through AQP2 on the apical side, through the cell, and exits via constitutively expressed AQP3 and AQP4 channels on the basolateral membrane into the interstitium and then into the bloodstream. R
This concentrates the urine and conserves body water.
When AVP levels fall, AQP2 channels are endocytosed (pulled back into the cell), the apical membrane becomes water-impermeable again, and dilute urine is excreted. R
Long-term AVP exposure also increases AQP2 gene transcription, amplifying the total pool of water channels available. R
Beyond AQP2, vasopressin also upregulates the urea transporter UT-A1 in the inner medullary collecting duct, which is required to maintain the medullary osmotic gradient that drives water reabsorption. R
Vasopressin And Overlapping Conditions
Vasopressin dysregulation intersects with many chronic conditions.
POTS And Dysautonomia
Many individuals with POTS have low blood volume (hypovolemia) and impaired vasoconstriction, both of which vasopressin normally helps correct. R
Inadequate AVP response during orthostatic challenge can worsen orthostatic tachycardia, and some POTS patients show blunted baroreflex-mediated AVP release. R
Salt and fluid loading (a first-line POTS recommendation) works in part by modulating osmolality-driven AVP release.
HPA Axis And Chronic Stress
AVP is a co-secretagogue for ACTH alongside CRH. R
Under acute stress, CRH dominates ACTH release, but during chronic or repeated stress, the balance shifts toward AVP-driven ACTH secretion. R
This is relevant in CRH resistance, where the CRH component of the HPA axis is downregulated but AVP-mediated ACTH drive may persist or increase.
Heart Failure
In congestive heart failure (CHF), non-osmotic AVP release is chronically elevated due to decreased effective circulating volume, even when plasma osmolality is normal or low. R
This drives pathological water retention, worsening edema and dilutional hyponatremia. R
V2 receptor antagonists (vaptans) like tolvaptan are used to promote free water excretion without sodium loss. R
Sepsis And Vasodilatory Shock
During septic shock, AVP stores in the posterior pituitary can become depleted after an initial surge, leading to inappropriately low AVP levels in the setting of severe hypotension. R
Exogenous vasopressin infusion at low doses (0.01 to 0.04 U/min) is used as a vasopressor adjunct in catecholamine-resistant vasodilatory shock. R
Autism And Social Behavior
AVP modulates social recognition, pair bonding, and aggression through V1a receptors in the brain. R
Children with autism spectrum disorder have been found to have lower cerebrospinal fluid vasopressin levels, with the degree of deficit correlating with severity of social impairment. R
Intranasal vasopressin has shown preliminary improvements in social communication in ASD clinical trials (although effects are modest and not yet standard of care). R
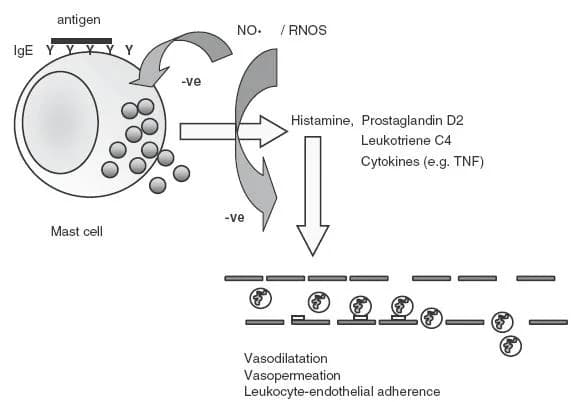
Mast Cell Activation
Mast cells express vasopressin receptors, and AVP can potentiate histamine release from mast cells, which may be relevant in individuals with Mast Cell Activation Syndrome (MCAS) who notice symptom flares related to fluid shifts, dehydration, or stress. R
How To Support Healthy Vasopressin Signaling
The goal is not to blindly raise or lower vasopressin, but to support the regulatory systems that keep it appropriate for context.
1. Hydration And Electrolyte Balance
Adequate hydration is the most fundamental regulator of AVP.
Chronic under-hydration drives sustained AVP elevation, which contributes to renal medullary stress and may accelerate chronic kidney disease progression. R
Overhydration (drinking far beyond thirst) suppresses AVP and can cause dilutional hyponatremia, particularly during endurance exercise.
For individuals with POTS, increasing sodium intake (2 to 3 grams of supplemental sodium per day with adequate water) helps maintain intravascular volume and modulates AVP release through osmolality signaling. R
Electrolyte powder with balanced sodium, potassium, and magnesium supports the osmotic environment in which AVP operates.
2. Sleep Hygiene
AVP follows a circadian pattern, with higher secretion during sleep to reduce urine production overnight (this is why nocturia can signal AVP insufficiency). R
Disrupted circadian rhythm impairs nocturnal AVP release.
Melatonin supplementation may indirectly support nocturnal AVP patterning by stabilizing the suprachiasmatic nucleus circadian clock. R
3. Blood Pressure Support
For individuals with low blood pressure and blunted AVP responses:
Licorice root (Glycyrrhiza glabra): inhibits 11-beta-hydroxysteroid dehydrogenase type 2, which increases cortisol availability at the mineralocorticoid receptor, promoting sodium and water retention (use with caution and monitoring, as it can raise blood pressure excessively in some individuals). R
Compression garments (20 to 30 mmHg waist-high) reduce venous pooling and improve baroreceptor afferent signaling, supporting appropriate AVP release during orthostasis.
4. Stress Axis Support
Because AVP is a co-regulator of the HPA axis, supporting appropriate stress responses matters.
Phosphatidylserine (300 to 800 mg/day) has been shown to blunt excessive ACTH and cortisol responses to stress, which may indirectly modulate the AVP-ACTH axis. R
Rhodiola rosea modulates the HPA axis at the level of CRH and cortisol without overly suppressing it. R
5. Omega-3 Fatty Acids
Omega-3 fatty acids (EPA/DHA) improve cell membrane fluidity, which affects receptor trafficking including AQP2 and V2R function. R
What To Stay Away From
Things that disrupt vasopressin signaling: (not exclusive list)
- Alcohol: ethanol directly inhibits AVP release from the posterior pituitary, which is why alcohol causes diuresis, dehydration, and contributes to hangover symptoms R
- Caffeine in excess: at high doses, caffeine may have a mild diuretic effect partly through AVP modulation (although moderate intake is generally well-tolerated and the diuretic effect is modest) R
- Chronic overhydration: drinking far beyond thirst suppresses AVP and can cause life-threatening hyponatremia (exercise-associated hyponatremia kills more marathon runners than dehydration) R
- Lithium: causes acquired nephrogenic DI by entering principal cells through ENaC channels and interfering with AQP2 trafficking (affects up to 40% of long-term lithium users) R
- SSRIs (can cause SIADH and hyponatremia, particularly in elderly patients, typically within the first few weeks of use) R
Testing
Blood And Urine Markers
Serum sodium: the most accessible indirect marker of AVP status (low sodium suggests excessive AVP or excessive water intake; high sodium suggests inadequate AVP or insufficient water intake). R
Serum osmolality: normal range 275 to 295 mOsm/kg, below this with concentrated urine suggests SIADH. R
Urine osmolality and specific gravity: inappropriately concentrated urine (above 100 mOsm/kg) when serum osmolality is low is diagnostic for SIADH. R
Copeptin: a stable surrogate biomarker for AVP (AVP itself is unstable and difficult to measure clinically). R
Basal copeptin above 21.4 pmol/L identifies nephrogenic DI. R
Stimulated copeptin below 4.9 pmol/L after hypertonic saline infusion diagnoses central DI. R
Comprehensive Panels
I use the Foundation Zoomer (Vibrant Wellness) to assess baseline sodium, CMP, and thyroid markers that influence fluid balance.
I use the Hormone Zoomer (Vibrant Wellness) to evaluate the broader hormonal context, including cortisol and DHEA, which co-regulate with AVP through the HPA axis.
I use the Cardio Zoomer (Vibrant Wellness) to assess metabolic markers, lipid profiles, and insulin signaling (insulin resistance can affect renal sodium handling).
For individual blood marker testing:
Comprehensive Metabolic Panel (Quest Diagnostics): includes serum sodium, potassium, chloride, BUN, creatinine, and glucose.
Fasting Insulin (Quest Diagnostics): insulin affects renal sodium reabsorption through ENaC, which interacts with AVP signaling.
Functional Testing
Water deprivation test: the gold standard for differentiating central DI from nephrogenic DI from primary polydipsia (must be done under medical supervision due to risk of severe dehydration). R
Hypertonic saline infusion with copeptin measurement: emerging as a more accurate diagnostic alternative to the water deprivation test. R
Mechanisms Of Action
Simple:
- AVP tells the kidney to hold onto water by inserting water channels into tubule cells
- AVP constricts blood vessels to raise blood pressure when volume is low
- AVP amplifies the stress hormone response by co-stimulating ACTH release from the pituitary
- The brain detects blood concentration (osmolality) and blood volume to decide how much AVP to release
- Alcohol blocks AVP release, which is why it makes you urinate more
Advanced:
- V2R-AQP2 Axis: AVP binding to V2R on the basolateral membrane of collecting duct principal cells activates Gs, stimulating adenylyl cyclase to generate cAMP, which activates PKA, phosphorylating AQP2 at serine-256 and triggering exocytic insertion of AQP2-bearing vesicles into the apical membrane, rendering it water-permeable. R
- V1a Vasoconstriction: V1a receptor activation on vascular smooth muscle couples to Gq/11, activating PLC-beta, hydrolyzing PIP2 to IP3 and DAG, releasing ER calcium stores and activating PKC, leading to myosin light chain phosphorylation and smooth muscle contraction. R
- V1b-ACTH Co-secretion: Parvocellular PVN neurons co-express CRH and AVP, which are co-released into the hypophyseal portal system and synergistically stimulate ACTH release from anterior pituitary corticotrophs via V1b (Gq-coupled) and CRH-R1 (Gs-coupled) receptors respectively, with AVP becoming the dominant ACTH secretagogue during chronic stress. R
- Osmoreceptor Transduction: Hypothalamic osmoreceptor neurons (in the organum vasculosum of the lamina terminalis and subfornical organ) are intrinsically osmosensitive via TRPV1 and TRPV4 channels, which detect cell volume changes and modulate firing rates of SON and PVN magnocellular neurons to calibrate AVP release. R
- Endosomal Signaling: The V2R continues to signal via Gs-beta-arrestin complexes after receptor internalization, generating sustained cAMP production from endosomes (a "mega-complex" that distinguishes V2R from most GPCRs, which terminate signaling upon internalization). R
Genetics
AVP (Arginine Vasopressin Gene)
The AVP gene (chromosome 20p13) encodes the prepro-vasopressin precursor, which is processed into the mature nonapeptide, neurophysin II, and copeptin. R
Mutations cause autosomal dominant familial neurohypophyseal diabetes insipidus (adFNDI), a progressive form of central DI where mutant precursor proteins misfold and accumulate in magnocellular neurons, eventually causing cell death. R
Over 70 distinct mutations have been identified, most in the neurophysin II moiety. R
AVPR2 (V2 Receptor Gene) — X-Linked
The AVPR2 gene is located on chromosome Xq28 and encodes the V2 receptor. R
Loss-of-function mutations cause X-linked nephrogenic diabetes insipidus, accounting for approximately 90% of hereditary NDI cases. R
Over 280 disease-causing variants have been catalogued. R
Because it is X-linked, males are fully affected while female carriers may have variable expressivity depending on X-inactivation patterns.
AQP2 (Aquaporin-2 Gene)
The AQP2 gene (chromosome 12q13) encodes the vasopressin-regulated water channel in the collecting duct. R
Mutations cause autosomal recessive or autosomal dominant nephrogenic DI, accounting for approximately 10% of hereditary NDI cases. R
Recessive mutations typically cause misfolding and ER retention of the AQP2 protein.
Dominant mutations produce AQP2 proteins that oligomerize with wild-type AQP2 and misdirect the complex away from the apical membrane.
AVPR1A (V1a Receptor Gene)
The AVPR1A gene (chromosome 12q14-15) encodes the V1a receptor involved in vasoconstriction, hepatic glycogenolysis, platelet aggregation, and social behavior. R
Promoter-region repeat length polymorphisms (RS1 and RS3 microsatellites) have been associated with variation in social behavior, pair bonding, musical creativity, and altruism in humans. R
rs3759292: associated with susceptibility to substance dependence in some populations. R
More Research
- AVP may have a direct role in regulating gut microbiome composition through effects on intestinal water secretion and motility (preliminary data). R
- Copeptin is emerging as a prognostic biomarker in acute myocardial infarction, with levels correlating to infarct size and mortality risk independently of troponin. R
- Elevated copeptin levels predict incident diabetes, likely reflecting chronic vasopressin-driven V1b stimulation of hepatic gluconeogenesis and V2-driven renal gluconeogenesis. R
- For biomarker testing of fluid balance, sodium status, and renal function, I use the Foundation Zoomer to assess the baseline metabolic panel, and the Cardio Zoomer for cardiovascular risk markers that intersect with vasopressin physiology.
- High water intake (above 2 liters per day) has been associated with lower copeptin levels and may reduce chronic kidney disease progression, supporting the hypothesis that chronic AVP elevation is nephrotoxic over time. R
- Intranasal AVP administration improves social cognition in healthy humans (enhanced recognition of emotional facial expressions and cooperative behavior) independently of its peripheral effects. R
- The interstitium acts as a sodium reservoir that modulates local osmolality and AVP signaling independent of plasma osmolality, which may explain why some individuals retain fluid without measurable changes in serum sodium. R
- Vasopressin receptor antagonists (vaptans) are being investigated as adjunctive therapy in autosomal dominant polycystic kidney disease (ADPKD), where tolvaptan has been shown to slow cyst growth and eGFR decline. R
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Electrolyte Complex
1 scoop/day
CoQ10
200mg/day
Magnesium Glycinate
400mg at bedtime