Benefits Of Rhodiola Rosea And Rhodiola Crenulata
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Rhodiola rosea and Rhodiola crenulata are two distinct adaptogenic plants from the same genus, with overlapping but not identical compound profiles, different traditional uses, and different bodies of clinical evidence behind them. In this post, we will discuss what each species is, how they differ, the documented benefits, the critical quality problem with commercial products, dosing, mechanisms of action, and genetics.
What Rhodiola Is
Rhodiola is a genus of perennial herbs in the family Crassulaceae with over 90 species worldwide, most growing at high altitudes in the Arctic, Siberia, Central Asia, and the Himalayan plateau. R
The genus has been used for centuries in traditional medicine across Scandinavia, Russia, China, and Tibet, with each culture emphasizing different species and applications. R
In modern research and supplement markets, two species dominate: Rhodiola rosea (golden root, Arctic root, roseroot), the subject of most Western clinical trials, and Rhodiola crenulata, listed in the Chinese Pharmacopoeia and used extensively in Tibetan and Chinese medicine for altitude sickness. R
Rhodiola rosea gets its name from the rose-like fragrance of the fresh-cut rhizome. It grows naturally in the Arctic regions of Europe and Asia (primarily Siberia and Scandinavia) and in the eastern coastal regions of North America, at high altitudes in dry, rocky soil and sea cliffs. R
The European Medicines Agency (EMA) approved a traditional-use herbal monograph for R. rosea in 2011 (EMA/HMPC/232091/2011), covering its use as an adaptogen for temporary relief of symptoms of stress, fatigue, exhaustion, and general weakness. R
This is a traditional-use classification, not a full efficacy registration, but it represents official regulatory recognition based on long-standing use and supporting clinical data.
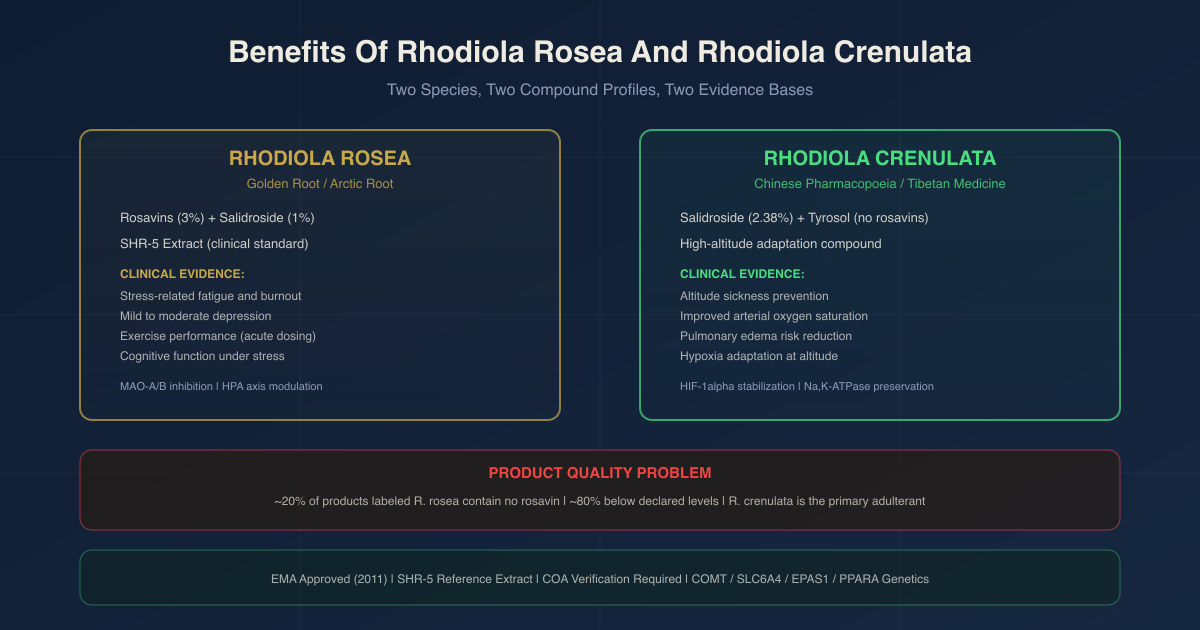
The SHR-5 extract is the standardized proprietary extract from the Swedish Herbal Institute (Gothenburg, Sweden) used in the majority of published clinical trials. It is standardized to rosavin 3.07% and salidroside 1.95%, reflecting the naturally occurring ratio of these compounds in authentic R. rosea. R
Rosea Vs Crenulata: Key Differences
These are two different plants with different phytochemical profiles, different traditional use contexts, and different bodies of evidence. They are frequently conflated in the supplement market, sometimes fraudulently. R
Rhodiola rosea:
- Primary compounds: rosavins (rosavin, rosarin, rosin, rhodiolin, rosiridin), salidroside (rhodioloside), tyrosol R
- Key marker: rosavins are unique to R. rosea within the Rhodiola genus; no other species contains them in significant quantity, making rosavin content the definitive marker of authentic R. rosea R
- Standard extract ratio: 3% rosavins : 1% salidroside, reflecting the naturally occurring 3:1 ratio in the plant R
- Primary traditional use: stress, fatigue, depression, physical endurance (Siberian, Scandinavian, and Eastern European traditions)
- Primary research use: mental fatigue, burnout, depression, exercise performance
- Regulatory status: EMA traditional-use monograph 2011; UK registered herbal medicinal product for stress-induced fatigue
Rhodiola crenulata:
- Primary compounds: salidroside, tyrosol, gallic acid (rosavins are absent or trace) R
- Key marker: high salidroside content with no rosavins; this is precisely why it is used to adulterate R. rosea products (lower cost, superficially similar) R
- Standard extract ratio: 2.38% salidroside and 0.44% p-tyrosol in studied clinical preparations R
- Primary traditional use: altitude sickness prevention in Tibet and Himalayan regions; listed in the Chinese Pharmacopoeia R
- Primary research use: acute mountain sickness (AMS), hypoxia adaptation
- Regulatory status: listed in the Chinese Pharmacopoeia; no Western regulatory approval
The two species are not interchangeable. R. rosea has the larger clinical evidence base for stress, fatigue, and mood. R. crenulata has the more targeted evidence base for altitude and hypoxia adaptation, driven primarily by its higher salidroside concentration. R
Both species also increased ATP content in mitochondria of skeletal muscles in a comparative study, though R. rosea showed stronger effects in that model. R
Benefits
1. Stress-Related Fatigue And Burnout (Rosea)
A phase III randomized, double-blind, placebo-controlled trial using SHR-5 extract (576 mg/day) in subjects with stress-related fatigue found significant improvements in burnout symptoms, fatigue, concentration, and cortisol awakening response over 28 days. R
In a study of 161 cadets (aged 19 to 21), a single dose of SHR-5 produced a pronounced antifatigue effect measured by the antifatigue index (AFI), a composite ratio of performance metrics, with the effect seen against a background of sleep deprivation and cognitive stress. R
In 56 Armenian physicians assessed during on-call night shifts, two weeks of R. rosea (standardized to 2.6% salidroside, 170 mg/day) produced significant improvement in a composite fatigue index compared to placebo. R
The EMA recognized these findings as supportive of the traditional-use claim for short-term fatigue and stress. R
2. Mild To Moderate Depression (Rosea)
A phase III, 6-week randomized, double-blind, placebo-controlled trial enrolled 89 patients with Hamilton Rating Scale for Depression (HAMD) scores of 21 to 31 (mild to moderate depression by DSM-IV criteria). R
Patients received SHR-5 at 340 mg/day, 680 mg/day, or placebo. Both active groups showed significant improvements in overall depression, insomnia, emotional instability, and somatization on HAMD scores compared to placebo. R
A 12-week randomized trial at the University of Pennsylvania compared R. rosea (SHR-5 extract, 340 to 1,360 mg/day), sertraline (50 to 200 mg/day), and placebo in adults with major depressive disorder (MDD). R
R. rosea produced a smaller antidepressant effect than sertraline but caused significantly fewer adverse effects, with a favorable tolerability profile. R
This is the expected finding for a mild-to-moderate indication: R. rosea is not positioned as a replacement for antidepressants in moderate to severe MDD, but as a lower-side-effect option in the mild-to-moderate range.
3. Exercise Performance And Ergogenic Effects (Rosea)
A 2024 review published in the British Journal of Nutrition identified at least 16 human investigations of R. rosea for exercise performance. R
Acute supplementation with approximately 200 mg of R. rosea (standardized to 1% salidroside and 3% rosavin) taken 60 minutes before exercise prolonged time-to-exhaustion and improved time trial performance in recreationally active adults. R
Recent trials with higher chronic doses (1,500 to 2,400 mg/day for 4 to 30 days) showed ergogenic effects during sprint cycling and resistance training in both trained and untrained adults. R
Evidence for R. rosea's effects on muscle damage, inflammation, and energy substrate use is currently equivocal, and chronic supplementation has shown more inconsistent results than acute dosing. R
4. Cognitive Performance Under Stress (Rosea)
In the cadet study above, the single-dose SHR-5 trial measured speed and accuracy of proofreading, mental arithmetic, perceptual and cognitive speed, and general mental performance. R
The antifatigue effect translated into measurable improvements in cognitive work capacity under conditions of sleep deprivation and stress, which is a more ecologically relevant test than rested cognitive function assessments. R
A pilot study of 10 participants with generalized anxiety disorder (GAD) taking 340 mg/day of R. rosea extract for 10 weeks found significant improvement in GAD symptoms measured by the Hamilton Anxiety Rating Scale, with reduction in scores comparable to those seen in psychopharmacological trials. R
(This is a small pilot study. The GAD finding is preliminary.)
5. Altitude Sickness Prevention And Treatment (Crenulata)
R. crenulata is the primary Rhodiola species used for altitude adaptation in traditional Chinese and Tibetan medicine. A randomized, double-blind, placebo-controlled crossover trial of R. crenulata extract (800 mg/day, standardized to 2.38% salidroside) taken 7 days before and 2 days during ascent from 250 m to 3,421 m found that R. crenulata did not significantly reduce the incidence of acute mountain sickness (AMS) as defined by a Lake Louise score ≥ 3 at this altitude and dosing protocol. R
The authors noted that participants did not reach altitudes where AMS is typically expected, and that active ingredients may have been lost during the extraction and purification process used in that study. R
Despite that null result for prevention in the crossover trial, a 2025 systematic review and meta-analysis of randomized controlled trials of R. crenulata extract for acute high altitude disease found that RCE was significantly more effective than placebo in improving arterial oxygen saturation (SaO2) and arterial partial pressure of oxygen (PaO2). R
RCE also appeared to perform as well as conventional Western medicine for improving blood oxygen levels in patients with established high altitude disease. R
The mechanism involves salidroside's ability to prevent hypoxia-mediated endocytosis of Na,K-ATPase from the plasma membrane of alveolar epithelial cells (via the ROS-AMPK-PKCζ pathway), preserving pulmonary sodium transport and reducing pulmonary edema risk at altitude. R
The Product Quality Problem
This section deserves its own space because it directly affects whether what you are buying has any relationship to what was studied in clinical trials.
A 2016 analysis by Booker et al. at University College London School of Pharmacy examined approximately 40 commercially available Rhodiola products from European suppliers. R
Results:
- Approximately one fifth of products claiming to contain R. rosea contained no rosavin at all (rosavin is unique to R. rosea and absent from all other Rhodiola species) R
- Seven samples were adulterated with other Rhodiola species or unknown material R
- Two samples appeared to contain no Rhodiola whatsoever R
- One sample was found to contain 5-HTP instead of Rhodiola R
- Approximately 80% of products with some rosavin content were still below the declared rosavin levels and appeared adulterated with other Rhodiola species R
A separate analysis found that none of the commercial dietary supplement products tested met their declared content of both rosavins and salidroside. R
R. crenulata is the primary adulterant because it is cheaper, grown more abundantly in China (listed in the Chinese Pharmacopoeia), contains salidroside (which partially mimics the marker compound profile), and lacks rosavin, making superficial identification difficult for buyers without HPTLC or NMR analysis. R
What to look for:
Products registered under the European Traditional Herbal Medicinal Products Directive (THMPD) or the UK's MHRA scheme were confirmed to be authentic R. rosea in the Booker analysis. The SHR-5 extract from the Swedish Herbal Institute is the reference standard extract used in clinical trials. Any product claiming standardization to 3% rosavins and 1% salidroside must be verified by a supplier who provides a certificate of analysis (COA) from third-party HPLC testing. There is no practical way for a consumer to verify authenticity without that documentation.
Rhodiola Rosea (standardized 3% rosavins / 1% salidroside)
Dosage And Safety
Rhodiola rosea:
The SHR-5 extract clinical trials have used doses ranging from 170 mg/day (fatigue study in physicians) to 680 mg/day (depression). R R
For stress and fatigue: 340 to 576 mg/day of a standardized extract (3% rosavins, 1% salidroside) is the range used in phase III trials. R
For exercise performance: acute dosing of approximately 200 mg taken 60 minutes before exercise is the best-supported protocol based on the available trials. R
R. rosea has a mild activating quality and is best taken in the morning or early afternoon, as taking it late in the day may interfere with sleep in sensitive individuals.
Adverse effects in clinical trials have generally been mild and infrequent, including headache, dizziness, and gastrointestinal upset. R
Rhodiola is not recommended alongside MAO inhibitors given its MAO-inhibiting pharmacology. R
Due to its cortisol-modulating effects, caution is warranted in people with adrenal insufficiency, or those on glucocorticoids.
Rhodiola crenulata:
The crossover AMS prevention trial used 800 mg/day taken 7 days before and 2 days during ascent. R
For altitude sickness applications: starting RCE supplementation 5 to 7 days before planned rapid ascent to high altitude is the protocol suggested by the trial data, with continuation during exposure.
No serious adverse events were reported in the RCT of R. crenulata. R
Mechanisms Of Action
Simple:
- Rhodiola inhibits monoamine oxidase A and B (MAO-A and MAO-B) in vitro, slowing the breakdown of dopamine, serotonin, and norepinephrine and supporting monoaminergic tone; this is the most mechanistically consistent explanation for its antifatigue and antidepressant effects R
- Salidroside modulates the hypothalamic-pituitary-adrenal (HPA) axis at the hypothalamic level, reducing stress-induced cortisol and ACTH secretion while preserving baseline adrenal function, which is the core adaptogenic mechanism R
- Rosavins contribute additional monoamine and glucocorticoid receptor modulation that is distinct from salidroside's HPA action, which is why the full extract with both compound classes may outperform single-compound preparations (preliminary data only) R
- For altitude: salidroside stabilizes HIF-1alpha (hypoxia-inducible factor 1-alpha) by blocking the enzymes that degrade it under hypoxic conditions, triggering a cellular hypoxia response that includes EPO induction and mitochondrial adaptation before symptoms occur R
- For exercise: Rhodiola modulates energy substrate use, reduces lactate accumulation post-exercise, decreases post-exercise muscle damage markers (creatine kinase, LDH), and increases skeletal muscle tissue oxygenation in animal models (animal and some human data) R
Advanced:
MAO inhibition and monoaminergic effects:
Ethanolic extracts of R. rosea roots inhibit both MAO-A and MAO-B in vitro. R
MAO-A preferentially catabolizes serotonin and norepinephrine; MAO-B preferentially catabolizes dopamine and phenylethylamine. By inhibiting both isoforms, R. rosea preserves monoamine availability in synaptic clefts. This is the same broad pharmacological class as non-selective MAOI antidepressants (phenelzine, tranylcypromine), though Rhodiola's MAO inhibition is far weaker and reversible, which is why it does not carry the tyramine ("cheese effect") food interaction risk associated with clinical MAOIs. However, combination with prescription MAOIs is inadvisable due to additive pharmacology.
Rhodiola also appears to modulate dopamine, serotonin, norepinephrine, and acetylcholine receptors in brain regions associated with affect and mood, though the receptor-level specificity is not fully characterized. R
HPA axis modulation:
Salidroside reduces the initial CRH (corticotropin-releasing hormone) release from the hypothalamus in response to stress, dampening the entire downstream HPA cascade. R
Lower CRH leads to reduced pituitary ACTH secretion, which reduces adrenocortical cortisol output. The adaptogenic relevance is that this modulation occurs specifically under stress conditions: basal adrenal function is preserved, meaning Rhodiola acts on the stress-induced component of HPA activation rather than suppressing the axis globally. This "stress-specific" modulation is characteristic of adaptogens as a pharmacological class and distinguishes them from glucocorticoids (which broadly suppress the axis regardless of context) and stimulants (which do not modulate cortisol at all). R
Rhodiola also modulates glucocorticoid receptors (GRs) directly, contributing to an anti-glucocorticoid effect that may underlie part of its neuroprotective and cognitive-preserving activity under chronic stress. R
HIF-1alpha stabilization (R. crenulata mechanism for altitude):
Under normoxia, prolyl hydroxylase domain proteins (PHDs) hydroxylate HIF-1alpha, targeting it for proteasomal degradation via the Von Hippel-Lindau (VHL) E3 ubiquitin ligase complex. Under hypoxia, PHD activity falls, HIF-1alpha accumulates, and it activates transcription of hypoxia-response genes including EPO (erythropoietin), VEGF, and genes governing mitochondrial energy metabolism. Salidroside inhibits targets in the HIF-1alpha degradation pathway, effectively mimicking the hypoxic stabilization of HIF-1alpha even before severe oxygen deprivation occurs. R
This preemptive HIF-1alpha stabilization activates the cellular hypoxia-response program before the organism reaches altitude, allowing partial acclimatization to begin prior to ascent. In addition, salidroside prevents hypoxia-induced endocytosis of the Na,K-ATPase alpha-1 subunit from alveolar epithelial cell membranes via ROS-AMPK-PKCζ signaling, maintaining the sodium pumps that keep alveolar fluid balance in check. R
Loss of alveolar Na,K-ATPase function under hypoxia impairs sodium reabsorption from the alveolar lining fluid, contributing to the pulmonary edema seen in severe AMS. By preserving Na,K-ATPase at the membrane, R. crenulata reduces this edema mechanism upstream.
AMPK and mitochondrial effects:
Salidroside activates AMPK (AMP-activated protein kinase) in some tissue and stress contexts, with downstream effects on mitochondrial biogenesis, fatty acid oxidation, and cellular energy sensing. R
Rhodiola extracts from both species activated ATP synthesis and resynthesis in mitochondria of skeletal muscle in a comparative study, with R. rosea showing stronger effects. R
(Note: AMPK activation by Rhodiola is context-dependent and bidirectional in some studies; the precise signaling outcomes differ between tissues and hypoxic versus normoxic conditions.)
Genetics
COMT (catechol-O-methyltransferase):
COMT catabolizes catecholamines (dopamine, norepinephrine, epinephrine) in the prefrontal cortex. The COMT Val158Met polymorphism (rs4680) determines COMT enzyme activity: Val/Val (high activity, faster catecholamine breakdown), Met/Met (low activity, slower breakdown), and Val/Met (intermediate). Individuals with Val/Val have lower prefrontal dopamine tone and are more sensitive to dopamine-modulating interventions. Given Rhodiola's MAO inhibition and monoaminergic effects, Val/Val carriers may show greater mood and cognitive benefit from R. rosea because they have more room for dopamine elevation in the prefrontal cortex from MAO inhibition. Met/Met carriers already have slower catecholamine breakdown and may be more prone to overstimulation at higher doses.
SLC6A4 (serotonin transporter):
The 5-HTTLPR promoter polymorphism in the serotonin transporter gene SLC6A4 affects serotonin reuptake efficiency. Short (S) allele carriers have reduced serotonin transporter expression and greater stress-induced serotonin dysregulation. Since Rhodiola's MAO-A inhibition increases serotonin availability in the synapse, S allele carriers under chronic stress may be disproportionate responders to R. rosea's serotonergic component.
EPAS1 / HIF2A and hypoxia-response genetics:
EPAS1 encodes HIF-2alpha, which works alongside HIF-1alpha in the hypoxia-response system. Tibetan populations carry specific EPAS1 variants (rs13419896, rs4953354) that are strongly associated with high-altitude adaptation and reduced hemoglobin concentration at altitude, representing one of the strongest examples of recent human natural selection. These variants alter HIF-2alpha stability and downstream EPO regulation. Individuals without these adaptations (essentially all lowlanders) have a more vulnerable HIF signaling system at altitude, which is the population most likely to develop AMS and for whom salidroside's HIF-1alpha stabilization is most relevant.
PPARA and fatty acid oxidation:
Rhodiola's AMPK-activating effects converge on PPARA (peroxisome proliferator-activated receptor alpha), which regulates genes governing fatty acid oxidation and mitochondrial energy substrate switching. Individuals with the PPARA Leu162Val variant (rs1800206) show altered fatty acid oxidation capacity and a different metabolic response to exercise stress, which may influence the magnitude of Rhodiola's ergogenic effects on substrate use and exercise efficiency.
More Research
- Long COVID and post-viral fatigue: A 2024 review proposed R. rosea alongside Ginkgo biloba as multi-target candidates for cognitive impairment and fatigue in post-COVID syndrome. R A quadruple-blind, randomized, placebo-controlled trial of adaptogens (including Rhodiola) for long COVID fatigue showed promising signals. The intersection of Rhodiola's HPA axis modulation, MAO inhibition, and mitochondrial effects with the post-viral fatigue phenotype is mechanistically plausible and warrants dedicated RCTs with long COVID endpoints.
- R. crenulata dosing and species gap in AMS prevention: The crossover RCT of R. crenulata for AMS prevention was conducted at altitudes (250 m to 3,421 m) where AMS incidence is moderate. R The 2025 meta-analysis found significant benefit for established high altitude disease. R The open question is whether higher doses, different species (R. rosea has been less studied for AMS), or decoction-form preparations (traditional Tibetan preparation) outperform the purified extract used in the negative crossover trial. The salidroside mechanism for alveolar Na,K-ATPase preservation is well-established at the cellular level; the dose and formulation question for humans remains open.
- The adulteration problem and regulatory gap: The scale of adulteration in the commercial Rhodiola market is severe enough to undermine any population-level interpretation of consumer supplement studies. R Until routine third-party verification of rosavin content becomes standard practice in the supplement industry, the gap between SHR-5 extract trial results and real-world supplement use will remain large. Consumers and clinicians should treat any R. rosea product without a verifiable COA showing rosavin and salidroside content as of unknown therapeutic value.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Methylated B Complex
1 cap/day with food
SAMe
400mg on empty stomach
Resveratrol
250mg/day