Histamine Intolerance vs MCAS: How to Tell Them Apart
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Histamine intolerance and mast cell activation syndrome cause overlapping flushing, hives, gut distress, and brain fog, which is exactly why they get confused for each other.
In this post, we will discuss what each condition actually is, the single mechanistic difference that separates them, how their symptoms overlap, how to test for each, the distinct protocols that address each one, and the genetics behind both.

The Basics: Defining Both Conditions
Both conditions involve too much histamine acting on the body, but they arrive there from opposite directions.
Histamine Intolerance
Histamine Intolerance (HIT) is an imbalance between the histamine load entering the body and the body's capacity to break it down. R
The histamine itself is normal.
The problem is degradation capacity, which depends mainly on two enzymes: Diamine Oxidase (DAO) and Histamine N-Methyltransferase (HNMT). R
DAO is the main enzyme that degrades histamine you eat, and it lives in the epithelial cells of the small intestine, the kidneys, the placenta, and the liver. R
HNMT is a cytosolic enzyme that degrades histamine made inside the body, including in the brain. R
When DAO activity is too low to clear the incoming load, histamine accumulates and produces migraines, gut symptoms, and allergy-like reactions without any true allergy being present. R
HIT is best thought of as a bucket overflowing, not a faucet stuck on.
Mast Cell Activation Syndrome
Mast Cell Activation Syndrome (MCAS) is the inappropriate, recurrent, episodic release of mast cell mediators into the body. R
The faucet here is the mast cell, and in MCAS it is releasing its contents when it should not.
Histamine is only one of those mediators.
Mast cells also release tryptase, Prostaglandin D2 (PGD2), leukotrienes, heparin, chemokines, and cytokines. R R
That broader mediator profile is why MCAS symptoms reach beyond what histamine alone explains, including anaphylaxis, bone pain, and pressure-driven flares.
To learn how mast cells behave at baseline before they misfire, see stabilizing mast cells.
The Key Difference
The central distinction is this: histamine intolerance is an enzyme and excess-load problem, while MCAS is a mast cell mediator-release problem.
In HIT, the cells are behaving normally and the degradation pathway is the bottleneck.
In MCAS, the degradation pathway may be fine and the cells themselves are the source.
This is why an MCAS patient can react to triggers that contain no histamine at all, such as heat, friction, pressure, exercise, or emotional stress, because those triggers cause mast cells to degranulate.
A pure HIT patient, by contrast, reacts in proportion to histamine intake and to anything that blocks DAO.
The practical consequence is that low-histamine eating and DAO support help HIT the most, while mast cell stabilization and mediator-receptor blockade help MCAS the most.
The two also coexist, because chronic mast cell activation raises the histamine load and can overwhelm DAO, producing HIT on top of MCAS.
How Each Mechanism Works
The Histamine Intolerance Mechanism
Histamine is synthesized from the amino acid histidine by the enzyme Histidine Decarboxylase (HDC). R
It also enters the body from aged, fermented, and microbially processed foods, and from histamine-producing gut bacteria. R
Under normal conditions DAO clears dietary histamine at the gut barrier before it reaches circulation. R
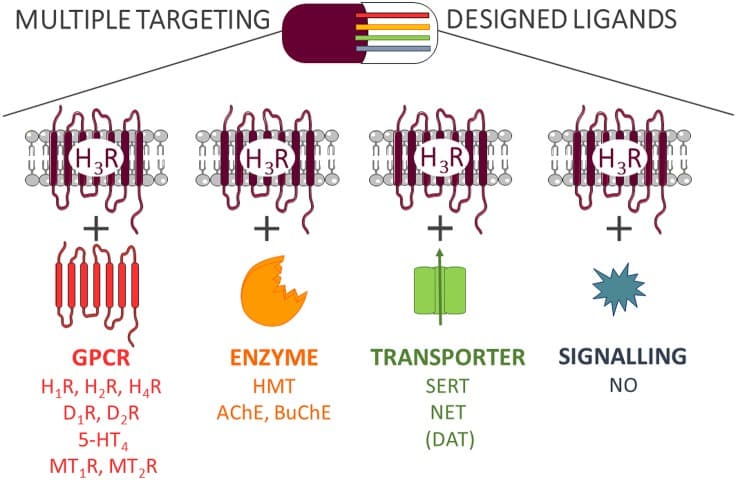
In HIT, DAO is insufficient, so histamine spills into plasma and acts on H1, H2, H3, and H4 receptors throughout the body. R
Other biogenic amines such as putrescine and cadaverine compete for the same enzymes and further saturate degradation, which is why a single trigger meal can tip someone over. R
Gut damage matters here, because DAO is produced by the intestinal lining, and a damaged lining produces less DAO.
This is the upstream reason dysbiosis and gut-barrier loss so often precede histamine problems.
The MCAS Mechanism
Mast cells are tissue-resident immune cells loaded with preformed granules and the machinery to synthesize lipid mediators on demand. R
When activated through IgE-bound FcεRI, the MRGPRX2 receptor, complement, neuropeptides like substance P, or physical triggers, they degranulate and release their full mediator set. R
In MCAS this activation threshold is set too low or the cells are intrinsically over-responsive, so they fire repeatedly and episodically. R
The released mediators act on multiple organ systems at once, which is built into the diagnostic definition requiring at least two organ systems involved. R
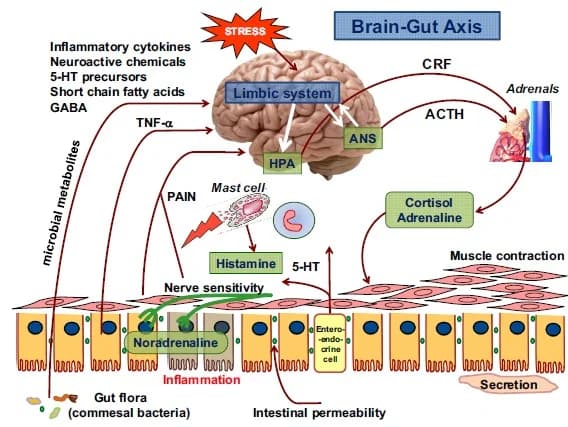
The nerve-to-mast-cell loop is a major driver, because sensory nerves release substance P, which degranulates nearby mast cells, which then sensitize the nerves further, as covered in substance P and neurogenic inflammation.
The Junction Dysfunction Framing
Within Jacob's Junction Dysfunction (JD) framework, mast cell behavior in chronic illness is not random, and this is Jacob's hypothesis rather than settled consensus.
Mast cells concentrate in connective tissue, which has a sparser capillary supply than other tissue.
When the glycocalyx is degraded and microcirculation is lost, those connective-tissue mast cells sit in hypoxic regions and degranulate histamine partly as an attempt to vasodilate and re-oxygenate the area, a mechanism detailed in mitochondria and mast cells in hypoxia.

This reframes MCAS as downstream of vascular and barrier damage rather than as a primary cell defect in a large subset of chronically ill patients.
It also links MCAS to Transient Capillary Leak Syndrome (TCLS), a term Jacob coined for the micro-scale capillary leak that drives fluid out of vessels and into tissue.
The HPA axis adds a second layer, because corticotropin-releasing hormone directly triggers mast cell degranulation, which is one reason stress flares are so consistent in these patients.
To go deeper on the barrier layer underneath all of this, see the glycocalyx and the JD chapter on Transient Capillary Leak Syndrome.
Overlapping Symptoms And How To Tell Them Apart
Both conditions can produce the same surface symptoms, which is the entire reason they get conflated.
Shared symptoms (present in both, not exclusive):
- Abdominal pain, bloating, diarrhea, and nausea
- Anxiety, brain fog, and insomnia
- Flushing and itching
- Headaches and migraines
- Hives and skin reactivity
- Nasal congestion and rhinitis
- Palpitations and lightheadedness on standing
The distinguishing features are what separate them in practice.
Features that point toward histamine intolerance (not exclusive):
- Reactions scale with histamine in food and improve on a low-histamine diet
- Reactions worsen with alcohol and DAO-blocking drugs
- Symptoms are dose-dependent and predictable from meals
- Symptoms often improve quickly with DAO supplementation R
Features that point toward MCAS (not exclusive):
- Anaphylaxis or near-anaphylaxis episodes
- Bone pain and pressure or friction urticaria
- Reactions to non-histamine triggers like heat, exercise, vibration, and emotional stress
- Symptoms involving two or more organ systems in discrete episodes R
- Triggering by medications acting on MRGPRX2, such as opioids and certain neuromuscular agents
The cleanest tell is trigger logic.
If your reactions track histamine load, lean HIT.
If your reactions fire on physical and emotional triggers that contain no histamine, lean MCAS.

How To Improve Each
The protocols share a foundation but diverge at the top, so they are split here by condition.
For Histamine Intolerance
1. Lower The Histamine Load
A low-histamine diet is the single most important intervention and is itself part of how the diagnosis is confirmed. R
It works by cutting both exogenous intake and the histamine-secreting gut bacteria that add to the load. R
Most patients improve but few reach total remission on diet alone, so it is a foundation rather than a cure. R
For the full food-by-food approach, see the 6-step histamine intolerance protocol.
2. Replace DAO Directly
Oral DAO taken before meals supplies the missing enzyme at the gut, and supplementation significantly improved symptom scores that returned when it was stopped. R
Diamine Oxidase (DAO) enzyme: Take 15 to 30 minutes before histamine-containing meals.
3. Supply The DAO Cofactors
DAO is a copper-dependent enzyme, and histamine degradation also depends on vitamin C and vitamin B6 status.
Vitamin C: Blood histamine rises as ascorbic acid falls, and supplementing it lowers blood histamine. R
- Copper (only if deficient, since excess is pro-oxidant) is the DAO metal cofactor
- Pyridoxal-5-Phosphate (active B6) supports DAO function
4. Repair The Gut That Makes DAO
Because DAO is produced by the intestinal lining, restoring the gut barrier restores DAO capacity over time.
This means addressing dysbiosis and choosing histamine-degrading rather than histamine-producing probiotic strains.
Bifidobacterium longum: A histamine-lowering strain preferable to histamine-producing lactobacilli in sensitive patients.
For MCAS
1. Stabilize The Mast Cell
Mast cell stabilizers reduce degranulation rather than blocking histamine after the fact.
Quercetin: A flavonoid that inhibited histamine and PGD2 release from human mast cells and outperformed cromolyn at blocking cytokine release. R
Luteolin: More potent than cromolyn at inhibiting release of histamine, tryptase, MMP-9, and VEGF from human mast cells, with strong neuroinflammation benefits. R R
The luteolin plus palmitoylethanolamide combination is covered in PeaLut and the mast cell-glia axis.
2. Block The Mediator Receptors
Combination H1 plus H2 antihistamine therapy covers a broader range of histamine receptors than either alone and is standard first-line MCAS management. R
Non-sedating H1 agents such as cetirizine, loratadine, and fexofenadine are paired with H2 agents such as famotidine.
Leukotriene receptor blockade addresses a mediator that antihistamines miss entirely. R
3. Add Prescription Stabilizers When Needed
Cromolyn sodium inhibits mediator release and is the most common maintenance add-on to antihistamines, with high-dose continuous oral regimens controlling symptoms in resistant cases. R R
This is a clinician-managed step, and a consultation is appropriate when over-the-counter stabilizers are not enough.
4. Address The Upstream Drivers
Because so much mast cell activation is driven from the nervous system and the gut, the durable fixes sit upstream.
Low gut serotonin and vagal dysfunction sensitize mast cells, as explained in gut serotonin and mast cell activation.
In the JD framing, repairing the glycocalyx and restoring microcirculation removes the hypoxic stimulus that makes connective-tissue mast cells degranulate.
What To Stay Away From
Some exposures worsen both conditions, and the avoid list is where the two protocols overlap most.
High-histamine foods and drinks (not exclusive):
- Aged cheeses and cured meats
- Alcohol, especially wine, champagne, and beer
- Fermented foods such as sauerkraut, kombucha, and soy sauce
- Leftover and slow-cooked protein that has aged in the fridge
- Smoked and canned fish
Histamine-liberating foods that trigger release without containing much histamine (not exclusive):
- Citrus fruits
- Shellfish
- Strawberries
- Tomatoes
DAO-blocking and mast cell-provoking drugs (discuss any prescription change with your clinician):
- Alcohol, which both adds histamine and blocks DAO
- Certain antibiotics and antiarrhythmics that inhibit DAO
- NSAIDs, which can trigger mast cell mediator release
- Opioids and some neuromuscular blocking agents, which activate MRGPRX2 on mast cells
For MCAS specifically, also limit non-chemical triggers where possible, including extreme heat, sudden temperature swings, mechanical pressure, and overexertion.
Testing
Testing separates the two conditions and rules out the more serious clonal mast cell disease that can masquerade as either.
Blood And Urine Markers
Plasma histamine reflects circulating histamine load and is most informative drawn during or shortly after a reaction.
I use the Histamine, Plasma test (Quest Diagnostics) to gauge histamine burden.
Serum tryptase is the central mast cell marker, and the consensus MCAS criterion is an event-related rise of at least 20% over the individual baseline plus 2 ng/mL within 4 hours of a reaction. R
I use the Tryptase test (Quest Diagnostics) for the baseline value, and a persistently elevated baseline above roughly 8 ng/mL raises suspicion for hereditary alpha-tryptasemia or clonal disease. R
Because a single timed tryptase often misses episodic activation, urinary mediator metabolites add diagnostic reach.
The major urinary PGD2 metabolite is a more sensitive index of in vivo mast cell activation than urinary N-methylhistamine, and either can confirm activation when tryptase is inconclusive. R
Urinary N-methylhistamine, the PGD2 metabolite, and leukotriene E4 are specialized 24-hour urine send-outs not yet in the lab store, so a consultation is the route to order and interpret them.
Functional Lab Panels
I use the Immune Zoomer (Vibrant Wellness) to assess mast cell-related markers and systemic autoantibodies that inform the MCAS picture.
I use the Gut Zoomer (Vibrant Wellness) to assess histamine-producing bacteria, zonulin-based barrier permeability, and the dysbiosis that suppresses DAO production, which is central to the HIT side.
I use the Nutrient Zoomer (Vibrant Wellness) to assess the copper, vitamin C, and vitamin B6 cofactors that DAO and histamine degradation depend on.
Individual cofactor markers are available as standalone tests, including Copper, Vitamin B6, and Vitamin C (all Quest Diagnostics).
For the overlapping dysautonomia picture, the POTS bundle combines cellular, hormone, gut, and neural panels.
Provocation And Elimination Testing
A structured low-histamine elimination followed by reintroduction is itself a diagnostic test for HIT, because a clear clinical response to histamine restriction is the strongest single confirmation of the diagnosis. R
Serum DAO activity can support the picture but should never be the sole basis for diagnosis, since low DAO correlates with but does not prove HIT. R
Mechanisms Of Action
Simple:
- Histamine intolerance is a clearance problem, where the body cannot break histamine down fast enough and it piles up.
- MCAS is a release problem, where mast cells dump histamine and many other chemicals when they should stay quiet.
- Both end with too much histamine acting on the body, which is why they feel similar.
Advanced:
- DAO insufficiency in HIT lets dietary histamine bypass intestinal degradation and reach systemic circulation, where it activates H1 through H4 receptors, and competition from other biogenic amines for DAO and HNMT compounds the saturation. R
- Mast cell hyper-releasability in MCAS lowers the activation threshold across FcεRI, MRGPRX2, complement, and neuropeptide pathways, releasing preformed histamine, tryptase, and heparin alongside newly synthesized PGD2 and leukotrienes across at least two organ systems. R R
- The hypoxia-degranulation link in Jacob's JD framing places connective-tissue mast cells in poorly perfused regions where glycocalyx loss and microcirculatory failure trigger histamine release as a vasodilatory rescue attempt, tying MCAS to TCLS rather than to a primary cell defect, which is his hypothesis and not consensus.
- HPA-driven degranulation through corticotropin-releasing hormone provides a stress-to-mast-cell pathway that explains emotional-trigger flares in MCAS independent of any histamine intake.
Genetics
AOC1
AOC1 encodes diamine oxidase, the principal enzyme that degrades extracellular and dietary histamine.
Variants in this gene reduce enzyme production or activity and are the dominant genetic contributor to histamine intolerance.
rs10156191 (Thr16Met), rs1049742 (Ser332Phe), and rs1049793 (His645Asp) each lower DAO activity, and a promoter variant rs2052129 reduces transcription. R
In one cohort, 79% of histamine-intolerant individuals carried at least one of these reduced-activity variants, and the effect is cumulative when several are present. R R
HNMT
HNMT encodes histamine N-methyltransferase, which degrades histamine inside cells, including in the central nervous system.
A functional variant reduces enzyme activity and slows intracellular histamine breakdown.
rs1801105 (C314T, Thr105Ile) lowers HNMT activity by up to roughly 50% and has been linked to asthma and atopic disease. R R
HDC
HDC encodes histidine decarboxylase, the enzyme that synthesizes histamine from histidine in mast cells, basophils, gastric cells, and specific neurons. R
Its expression is controlled largely by promoter methylation rather than by common coding variants, so upregulation of HDC raises histamine production on the supply side. R
This is the synthesis counterpart to the degradation problems in AOC1 and HNMT.
TPSAB1 (Highest Relevance For Tryptase)
TPSAB1 encodes alpha-tryptase, and its copy number defines hereditary alpha-tryptasemia, a common autosomal dominant trait.
Hereditary Alpha-Tryptasemia (HaT) is defined by extra copies of the alpha-tryptase allele, raises baseline serum tryptase, and affects roughly 5 to 6% of some populations. R
Increased TPSAB1 copy number associates with flushing, gastrointestinal symptoms, connective-tissue abnormalities, and autonomic dysfunction, and it is best quantified by droplet digital PCR rather than standard genotyping. R R
HaT matters because it explains a high baseline tryptase that would otherwise be read as clonal mast cell disease, and it overlaps heavily with the POTS-hEDS-MCAS picture.
More Research
For biomarker testing I use the Histamine, Plasma and Tryptase tests (Quest Diagnostics) for the two core markers, and the Immune Zoomer (Vibrant Wellness) for the broader mast cell and autoantibody picture.
Clonal mast cell disease such as systemic mastocytosis driven by the KIT D816V mutation must be excluded before settling on MCAS, because the treatment and prognosis differ sharply, and elevated baseline tryptase is the usual prompt to look. R
The overlap between POTS, hypermobile Ehlers-Danlos syndrome, and MCAS is now widely reported, with about a quarter of patients in some cohorts carrying all three labels, though the literature still debates whether the association reflects shared causation or definitional overlap. R R
This triad maps onto Jacob's JD framework as connective-tissue fragility, Vaso-Adaptive Disorder (VAD), and mast cell degranulation all emerging from glycocalyx and microcirculatory failure, which is his hypothesis rather than established science, and the POTS root causes and connective tissue disorder posts develop it further.
Vitamin C is worth flagging twice, because the inverse relationship between blood ascorbate and blood histamine means low vitamin C status can quietly raise the histamine baseline in both conditions, and intravenous ascorbic acid lowered serum histamine in allergic and infectious patients. R R
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Quercetin
500mg 2x/day
Vitamin D3 + K2
5000 IU + 200mcg/day
DAO Enzyme
1 cap before meals