Chapter 33
Chapter 33 of 47
By Jacob Gordon, INHC, FMT-C
6 min readPath Guide
When Your Innate Immune System Doesn’t Work, You Must Rely on the Adaptive Immune System
When the immune system first fights something, the first line of defense is the innate immune system.
The Innate Immune System, the Glycocalyx, and Tight Junctions
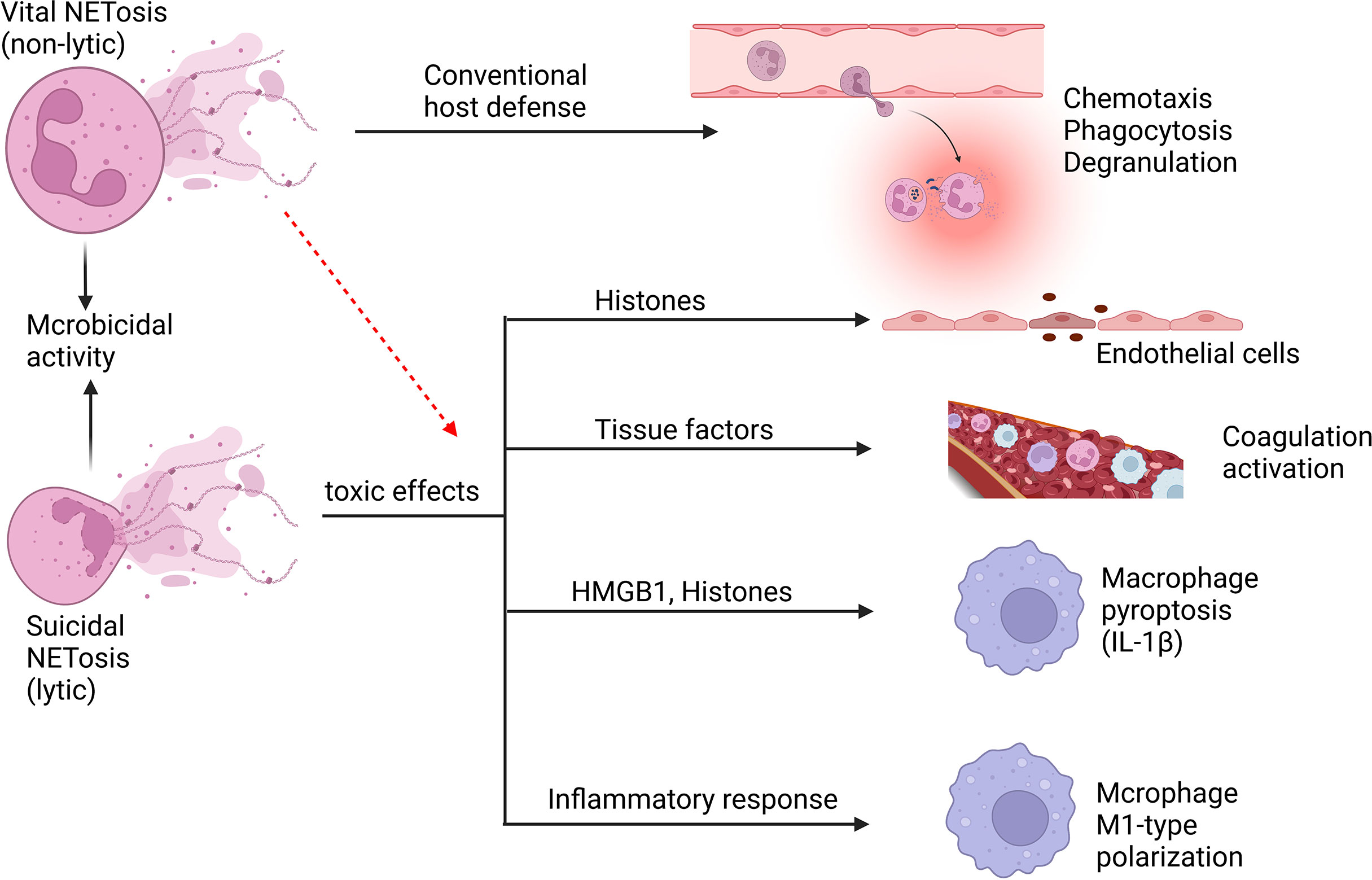
Neutrophils and NETs
Neutrophils (NTs) are part of the innate immune system that are responsible for killing pathogens on the spot.
End of Chapter 33
Up Next
Unlock with Path