Interstitial Cystitis / Bladder Pain Syndrome: Root Causes Beyond The Bladder
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Interstitial cystitis is a chronic bladder pain condition that is rarely about the bladder alone, which is why so many people fail antibiotics, instillations, and surgery before they ever address the real drivers.
In this post, we will discuss what interstitial cystitis actually is, the two distinct phenotypes, the defective protective barrier hypothesis, the central role of mast cells and neurogenic inflammation, the conditions that overlap with it, a root-cause protocol, what to avoid, how to test, the mechanisms, and the genetics.

Basics Of Interstitial Cystitis
Interstitial Cystitis (IC), also called Bladder Pain Syndrome (BPS), is a chronic condition of bladder pain, pressure, or discomfort that worsens with bladder filling and is associated with urinary urgency and frequency, in the absence of infection or other identifiable cause.
It is not a urinary tract infection, even though it feels like one that never resolves.
The defining experience is pain that builds as the bladder fills and eases briefly after voiding, often with daytime frequency, nocturia, and pelvic pain that radiates to the urethra, vagina, perineum, or low back.
IC/BPS splits into two phenotypes that behave like different diseases.
- Hunner lesion IC is the inflammatory subtype, defined by reddened mucosal lesions seen on cystoscopy, with epithelial denudation, dense immune infiltration, and a proven bladder-localized etiology. R
- Non-Hunner BPS is the far more common subtype, lacks those lesions, shows little evidence of primary bladder pathology, and behaves much more like a systemic pain-processing disorder. R
The Hunner subtype tends to appear in older patients, with greater frequency, more nocturia, and smaller bladder capacity, and is reported in roughly 5 to 57 percent of cohorts depending on how aggressively cystoscopy is used. R
This distinction matters because the two phenotypes respond to completely different interventions, and treating non-Hunner BPS as if it were a bladder lesion is one reason conventional care so often fails. R
This post is the bladder-focused companion to my deeper write-up on prostatitis and chronic pelvic pain syndrome, which shares most of the same machinery.
What Causes Interstitial Cystitis
There is no single cause, and that is the entire point.
IC/BPS is best understood as a final common pathway that several upstream insults converge on.
Root contributors (not an exclusive list):
- Bladder lining barrier breakdown where the protective sugar coat thins and lets urine solutes reach the bladder wall. R
- Central sensitization where the spinal cord and brain amplify normal bladder signals into pain. R
- Genetic susceptibility clustering in families alongside other chronic pain disorders. R
- Mast cell activation in the bladder wall releasing histamine, tryptase, and inflammatory mediators. R
- Neurogenic inflammation where sensory nerves and mast cells drive each other in a loop. R
- Pelvic floor dysfunction where chronically tight, tender muscles refer pain into the bladder. R
In most non-Hunner patients, the bladder is the screen the symptom is projected onto, not the projector.
The drivers sit upstream in the nervous system, the immune system, the pelvic floor, and the gut.
How The Bladder Lining Fails
The inner surface of the bladder is coated by a layer of glycosaminoglycans (GAGs), the same family of negatively charged, sulfated sugars that make up the protective coats on blood vessels and other epithelial surfaces.
This bladder GAG layer is built from chondroitin sulfate, heparan sulfate, hyaluronic acid, and keratan sulfate, and it sits on top of the urothelium, the specialized cell layer that lines the bladder. R
In a healthy bladder, this coat acts as a barrier that keeps the high-potassium, acidic, solute-rich urine from reaching the underlying cells and nerves.
The leading mechanistic hypothesis is that in IC/BPS the GAG layer becomes defective and permeable, allowing urinary solutes, especially potassium, to leak into the bladder wall, depolarize sensory nerves, and trigger inflammation and mast cell degranulation. R
This is the basis of the potassium leak model and the older potassium sensitivity provocation test.
There is a big MAYBE here.
At least one electron microscopy study found no consistent difference in the glycocalyx or urothelial appearance between IC patients and controls, so the leaky barrier is a strong working model rather than settled fact. R
Once the barrier is compromised, the bladder wall recruits and activates mast cells.
Mast cell counts run roughly 6 to 8 fold higher in the detrusor muscle in classic Hunner IC, and 2 to 3 fold higher in non-ulcerative BPS, and these cells activate even without obvious degranulation. R
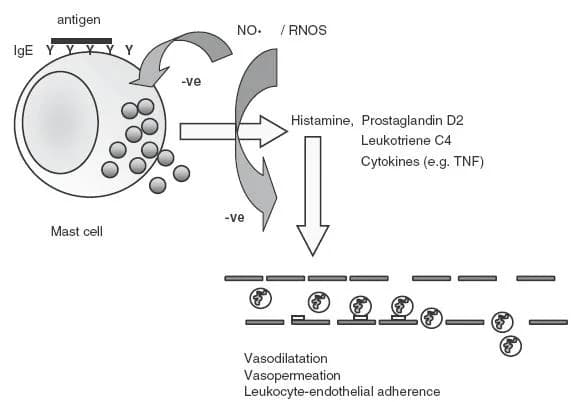
Activated bladder mast cells release histamine, tryptase, and vasoactive mediators that sensitize nearby sensory nerves.
Those sensitized nerves release substance P and other neuropeptides, which in turn degranulate more mast cells, closing a self-reinforcing neurogenic inflammation loop. R

This nerve-to-mast-cell loop is the same circuit I describe in mast cells, substance P, and neurogenic inflammation, just localized to the bladder.
There is also a wound-healing signature.
IC urine shows elevated antiproliferative factor (APF), a peptide that blocks bladder epithelial cells from proliferating, alongside reduced heparin-binding epidermal growth factor-like growth factor (HB-EGF), the growth signal those cells need to repair. R
APF directly suppresses HB-EGF signaling, which means the bladder lining is simultaneously being damaged and being told not to heal. R

A Junction Dysfunction View
This is where the bladder story connects to my broader Junction Dysfunction (JD) framework.
JD is my umbrella term for what happens when the glycocalyx, the sulfated sugar barrier that coats endothelial, epithelial, and immune cell surfaces, becomes compromised and lets fluid, ions, and toxins cross barriers they should not.
The bladder GAG layer is a glycocalyx-class barrier built from the exact same sulfated sugars (heparan sulfate, chondroitin sulfate, hyaluronic acid) that I write about in the glycocalyx and rebuilding the glycocalyx.
My hypothesis is that the bladder lining failure in IC/BPS is the urological face of the same cascade I describe systemically, where mast cells and other immune cells release heparanase, hyaluronidase, and matrix metalloproteinases (MMPs) that shed the sulfated barrier, expose the tissue beneath, and open the door to solute leak and neurogenic inflammation.
In that framing, the potassium leak across a damaged bladder GAG layer is a localized version of Transient Capillary Leak Syndrome (TCLS), the micro-level barrier leak I coined to describe how a degraded glycocalyx lets fluid and ions cross where they should not. R
I want to be clear that the bladder-as-TCLS connection is my hypothesis, not established urology, and I offer it as a way to think about why barrier repair and mast cell stabilization tend to help.
The deeper mechanistic chain (heparanase shedding, mast cell mediators, sulfation chemistry) is covered in the Junction Dysfunction guide.
Interstitial Cystitis And Overlapping Conditions
IC/BPS rarely travels alone, and the company it keeps tells you it is a systemic pain-processing problem.
In a large case-control study, self-reported comorbid diagnoses in IC/BPS versus controls were irritable bowel syndrome 38.6 versus 5.2 percent, fibromyalgia 17.7 versus 2.6 percent, and chronic fatigue syndrome 9.5 versus 1.7 percent. R
As the number of overlapping conditions rises, pain, depression, sleep disruption, and quality of life all get worse. R
Conditions that overlap with IC/BPS (not an exclusive list):
- Chronic fatigue syndrome / ME-CFS as part of the central sensitization cluster. R
- Fibromyalgia, a widespread pain disorder, co-occurring far above population rates. R
- Irritable bowel syndrome (IBS), reflecting shared visceral hypersensitivity. R
- Mast cell activation syndrome (MCAS), given the shared mast cell biology. R
- Prostatitis and chronic pelvic pain syndrome, the male-pattern counterpart. R
- Vulvodynia, which shares neurogenic inflammation and central sensitization pathways with IC/BPS. R
The thread running through all of these is central sensitization, where the nervous system turns up the gain on normal signals until ordinary bladder filling, gut motility, or light touch register as pain. R
The mast cell is the other shared thread, which is why so many IC patients also recognize themselves in my writing on why histamine produces so many symptoms and gut serotonin and mast cell activation.
If your bladder pain sits inside a wider web of gut, pain, and histamine symptoms, the bladder is unlikely to be the place to start.
How To Improve Interstitial Cystitis
The logic here is to repair the barrier, calm the mast cells, downshift the sensitized nervous system, release the pelvic floor, and remove the dietary triggers, all at once.
This is a layered protocol, not a single magic bullet, and the phenotype matters.
Work with a clinician who knows IC/BPS, and if you want help building a personalized version of this, that is what consultations are for.
1. Rebuild The Bladder GAG Layer
The most direct barrier-repair tools supply the same sulfated sugars the bladder coat is made of.
Glucosamine Chondroitin:
Oral chondroitin sulfate and glucosamine supply GAG building blocks, and intravesical hyaluronic acid plus chondroitin sulfate instillations are used clinically to resurface the barrier. R
Aloe Vera:
Concentrated oral aloe vera is rich in mucopolysaccharides and is a long-standing IC community staple, with a large patient survey reporting symptom relief and an FDA-cleared randomized trial underway, though peer-reviewed controlled data is not yet published.
Marshmallow Root:
A demulcent herb traditionally used to soothe irritated mucosal surfaces of the urinary tract.
The pharmaceutical version of this strategy is oral pentosan polysulfate, the only FDA-approved oral IC drug, which works modestly as a synthetic GAG analog but carries a now well-documented risk of pigmentary maculopathy with long-term cumulative dosing. R
2. Stabilize Mast Cells And Lower Histamine
Quercetin:
Quercetin is a mast cell stabilizing bioflavonoid, and in a double-blind placebo-controlled trial in category III chronic pelvic pain it produced a 35 percent improvement in symptom scores versus 7.2 percent for placebo. R
Luteolin:
A flavonoid that stabilizes mast cells and calms microglia, often paired with quercetin and with PEA.
Palmitoylethanolamide:
Palmitoylethanolamide (PEA), an endogenous lipid that downregulates mast cell activation along the mast cell-glia axis, reduced pain progressively over 6 months when given as micronized PEA-polydatin in IC/BPS patients. R
PEA and luteolin are the same combination I cover in my post on PeaLut and the mast cell-glia interaction.
3. Downshift Central Sensitization
Because non-Hunner BPS is largely a pain-processing disorder, calming the nervous system is not optional.
The most effective levers here are the same ones I emphasize for any centrally sensitized condition.
- Limbic and nervous system retraining (meditation, NLP, brain retraining programs) to lower the threat signal the brain assigns to bladder sensation.
- Magnesium and L-theanine to support NMDA tone and parasympathetic balance.
- Sleep repair, since poor sleep amplifies pain and IC frequency feeds insomnia.
Magnesium Glycinate:
A well-tolerated magnesium form that supports NMDA receptor modulation and muscle relaxation, including the pelvic floor.
4. Release The Pelvic Floor
A chronically tight, tender pelvic floor refers pain directly into the bladder and urethra and is one of the most underdiagnosed drivers.
In a randomized multicenter trial, ten sessions of myofascial pelvic floor physical therapy produced a 59 percent response rate versus 26 percent for general therapeutic massage in women with IC/BPS and pelvic floor tenderness. R
Find a pelvic floor physical therapist who does internal myofascial trigger point release, not generic Kegels, which can make a hypertonic floor worse.
5. Fix The Gut And Identify Food Triggers
The IBS overlap is not a coincidence, and the gut-bladder axis runs both ways.
Addressing dysbiosis and intestinal permeability lowers the systemic inflammatory and histamine load that keeps bladder mast cells primed.
A structured elimination diet for at least a month, followed by careful reintroduction, is the most reliable way to find your personal bladder irritants, since nearly 90 percent of IC patients report food sensitivities. R
Calcium Glycerophosphate:
An over-the-counter acid-buffering supplement that patient surveys identify as one of the few products that reduces symptoms when taken with trigger foods. R
6. A Note On D-Mannose
D-Mannose:
D-mannose is for bacterial UTIs, where it blocks E. coli adhesion to the bladder wall, and it is not an IC treatment, though many IC patients use it because IC flares mimic infection.
Be honest about its limits, because a recent large randomized trial found daily D-mannose did not significantly reduce medically attended UTIs versus placebo in women with recurrent UTI. R
It is worth keeping on hand to rule infection in or out, not as a barrier-repair tool.
What To Stay Away From
The most consistently reported bladder irritants come from questionnaire studies of IC patients, and removing them is often the single highest-yield first step. R
Common dietary triggers (not an exclusive list):
- Alcohol and carbonated beverages
- Artificial sweeteners
- Citrus fruits and juices
- Coffee, tea, and other caffeine
- Spicy foods
- Tomatoes and tomato products
- Vitamin C in high supplemental doses (ascorbic acid form)
A few non-dietary cautions matter too.
- Avoid reflexively retaking antibiotics for every flare when cultures are negative, since IC is not an infection and repeated courses worsen dysbiosis.
- Avoid pushing through with aggressive exercise during a flare, since pelvic floor overload and systemic inflammation can intensify symptoms.
- Be cautious with long-term high-dose pentosan polysulfate given the maculopathy risk, and get regular retinal screening if you use it. R
Testing
The goal of testing is to confirm the diagnosis, rule out mimics, identify the phenotype, and map the upstream drivers.
Imaging And In-Office Procedures
Cystoscopy with hydrodistension under anesthesia is used to identify Hunner lesions and assess bladder capacity, and is the main tool that separates the two phenotypes. R
The potassium sensitivity test (intravesical potassium provocation) has historically been used to probe a leaky GAG layer, but it is uncomfortable and has fallen out of favor due to poor specificity. R
Blood And Urine Markers
A clean urinalysis and culture are essential first to exclude infection, since IC is a diagnosis of exclusion.
I use the Foundation Panel (Vibrant Wellness) for a baseline CBC, metabolic panel, and inflammatory markers to rule out systemic disease.
For mast cell involvement, I use Plasma Histamine (Quest) and Tryptase (Quest) to assess mast cell burden, recognizing that bladder-localized mast cell activity can be present with normal systemic levels. R
Functional Lab Panels
I use the Immune Panel (Vibrant Wellness) to assess systemic autoantibodies and mast cell markers in patients with multisystem symptoms.
I use the Gut Panel (Vibrant Wellness) or the GI-MAP (Diagnostic Solutions) to assess dysbiosis, intestinal permeability, and the IBS overlap that keeps bladder mast cells primed.
I use the Food Sensitivity Panel (Vibrant Wellness) to narrow down dietary triggers alongside a structured elimination diet. R
For patients with a histamine and hormone pattern, especially where vulvodynia overlaps, I use the Hormone Panel (Vibrant Wellness) or the DUTCH Complete (Precision Analytical) to assess estrogen and cortisol rhythm.
Where mold or chemical exposure is plausible, I use the Toxin Panel (Vibrant Wellness) to assess mycotoxins and environmental chemical body burden.
Provocation And Elimination Testing
A monitored elimination diet for a minimum of one month, with single-food reintroduction, is the most practical provocation test for identifying personal bladder irritants. R
Mechanisms Of Action
Simple:
- The protective sugar coating on the inside of the bladder wears thin, so irritating urine reaches the raw tissue and nerves underneath and triggers pain.
- Immune cells called mast cells flood the bladder wall and dump histamine and other chemicals that inflame nerves.
- Those irritated nerves and mast cells egg each other on in a loop, and over time the spinal cord and brain learn to treat normal bladder filling as pain.
Advanced:
- GAG barrier permeability The apical urothelial GAG layer (chondroitin sulfate, heparan sulfate, hyaluronic acid, keratan sulfate) normally blocks transmural diffusion of urinary solutes, and its disruption permits potassium influx into the interstitium, depolarizing sensory afferents and provoking inflammation and mast cell degranulation. R
- Mast cell-driven neurogenic inflammation Detrusor and suburothelial mastocytosis with mast cell activation releases histamine, tryptase, and TNF, which sensitize C-fiber afferents that release substance P and CGRP, which further degranulate mast cells in a self-amplifying loop. R
- APF and HB-EGF dysregulation Urinary antiproliferative factor, a frizzled-8 related sialoglycopeptide, inhibits urothelial proliferation and suppresses HB-EGF-driven Erk/MAPK signaling, impairing barrier repair and locking the urothelium in a damaged, non-healing state. R
- Central sensitization Quantitative sensory testing, functional MRI, and widespread pain phenotyping demonstrate amplified central pain processing in IC/BPS, shared with fibromyalgia, IBS, and vulvodynia, explaining why peripheral bladder-only therapies frequently fail. R
Genetics
IC/BPS aggregates in families and shares genetic architecture with other chronic pain and mood disorders, which is why it should be thought of as a heritable sensitization trait, not a random bladder accident.
First-degree relatives of IC patients carry the diagnosis far more often than the general population, and concordance is higher in identical than fraternal twins. R
Nociplastic Pain Susceptibility
Family studies show multi-generational aggregation of IC together with other nociplastic pain disorders, depression, and panic disorder, pointing to shared inherited pain-processing biology rather than a single bladder gene. R
Hunner-Type IC And Autoimmunity
A genome-wide cross-trait analysis in East Asian populations identified shared genetic basis and causal relationships between Hunner-type IC and autoimmune diseases, supporting the view that the Hunner subtype is a distinct, more autoimmune-flavored disease. R
For the sulfation and redox genes that govern glycocalyx and GAG integrity more broadly (SUOX, CBS, SOD2), see the genetics layer of the Junction Dysfunction guide, since the same sulfur chemistry that builds heparan and chondroitin sulfate builds the bladder coat.
More Research
A few threads are worth watching and add genuine value beyond the protocol.
- Aloe vera for IC is moving from survey data toward real evidence, with an FDA-cleared randomized controlled trial of concentrated oral aloe vera underway, so the next few years should clarify whether the community experience holds up.
- APF and HB-EGF remain the most specific candidate urine biomarkers for IC, present in over 90 percent of clinically diagnosed patients, and may eventually allow diagnosis without cystoscopy. R
- For biomarker and pattern tracking over time, I use the Immune Panel and Gut Panel to follow mast cell and dysbiosis markers as the protocol takes effect, and members can log symptoms and lab trends in the Health Hub.
- Phenotype-directed care is the real frontier, since lumping Hunner and non-Hunner IC together has buried treatment signals for decades, and the Hunner subtype responds to lesion-directed therapy while non-Hunner BPS responds to systemic pain and pelvic floor work. R
- The bladder GAG layer as a glycocalyx-class barrier is, in my framing, the urological window into Junction Dysfunction, and I think barrier repair plus mast cell stabilization will keep outperforming bladder-only approaches as the evidence matures.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Electrolyte Complex
1 scoop/day
CoQ10
200mg/day
Magnesium Glycinate
400mg at bedtime