Pacing And Energy Management For ME/CFS And Long COVID
By Jacob Gordon, INHC, FMT-CPost-Exertional Malaise (PEM) is the defining feature of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and a central driver of disability in long COVID, yet most patients are never taught how to manage it.
In this post, we will discuss what PEM actually is at the mechanistic level, the energy envelope model of pacing, practical strategies for managing physical and cognitive exertion, heart rate monitoring, crash recovery protocols, overlapping conditions, testing, and the junction dysfunction biology behind exercise intolerance.

Basics Of ME/CFS And PEM
ME/CFS is a complex, multisystem neuroimmune disease affecting an estimated 17 to 24 million people worldwide, with fewer than 10 percent diagnosed. R
The hallmark symptom is Post-Exertional Malaise (PEM), defined as a disproportionate worsening of symptoms after physical, cognitive, or emotional exertion that would have been well tolerated before the illness. R
PEM is not fatigue in the ordinary sense.
It is a delayed, prolonged exacerbation of the full symptom complex, often hitting 12 to 48 hours after the trigger and lasting days, weeks, or longer. R
Patients describe it as crushing exhaustion, flu-like body aches, brain fog, orthostatic intolerance, sensory hypersensitivity, and a feeling of being poisoned or "hit by a truck."
The key distinction between PEM and normal post-exercise soreness is that PEM is not proportional to the effort expended and does not resolve with rest within a normal recovery window. R
This is the single feature that separates ME/CFS from primary depression, deconditioning, or simple fatigue syndromes.
Graded exercise therapy and "push through the fatigue" approaches harm this population.
Multiple studies show that exercise intervention programs that fail to account for PEM worsen outcomes, trigger relapses, and reduce long-term functioning. R
PEM And Long COVID
A significant subset of long COVID patients, estimated at 30 to 50 percent of those who meet criteria for Post-Acute Sequelae of SARS-CoV-2 (PASC), develop a PEM phenotype clinically indistinguishable from ME/CFS. R
Two-day Cardiopulmonary Exercise Testing (CPET) studies in both populations show the same pattern of objective decline on day two, suggesting a shared mechanism of impaired post-exertional recovery. R
I treat these two groups identically when it comes to pacing and energy management.
What Causes Post-Exertional Malaise
PEM is caused by a failure of energy systems to recover after exertion, not by deconditioning or fear of activity.
The largest two-day CPET study to date, published in 2024 with 84 ME/CFS patients and 71 controls, showed that patients failed to reproduce their day one exercise measures on day two, with significant declines in oxygen consumption, workload, heart rate, oxygen pulse, and ventilatory efficiency. R
These declines persisted when patients were matched to controls for aerobic capacity, proving that fitness level does not explain the phenomenon. R
Mitochondrial Dysfunction And The M1 State
Mitochondria in ME/CFS are stuck in a pro-inflammatory, pro-oxidative state that Jacob terms the Mitochondrial M1 State.
Instead of shifting between metabolic modes based on demand, these mitochondria remain locked in a high-output inflammatory configuration that generates excessive reactive oxygen species and fails to produce adequate ATP. R
This is covered in depth in the Mitochondria And Mast Cells In Hypoxia chapter of the JD guide.
The Wiskott-Aldrich Syndrome Protein Family Member 3 (WASF3) protein is overexpressed in ME/CFS muscle tissue, disrupting mitochondrial respiratory supercomplex formation and reducing complex IV levels. R
Endoplasmic reticulum stress drives WASF3 expression, creating a self-reinforcing loop: exertion triggers ER stress, which increases WASF3, which impairs mitochondrial respiration, which makes the next exertion more damaging. R
ANGPT2 And Endothelial Dysfunction
Angiopoietin-2 (ANGPT2) is elevated in ME/CFS and long COVID, consistent with ongoing glycocalyx loss and endothelial junction instability. R
When the glycocalyx becomes degraded, the ANGPT/TIE2 signaling axis destabilizes, leading to further heparanase release and more glycocalyx shedding in what Jacob describes as a bidirectional destabilization loop.
This is detailed in Junction Dysfunction And Transient Systemic Capillary Leak Syndrome.
The practical consequence is that the microcapillary network cannot deliver oxygen to working muscle and brain tissue at the rate required during exertion, forcing early reliance on anaerobic metabolism and generating lactate at lower workloads.

TGFB-Driven Circadian Uncoupling
Transforming Growth Factor Beta (TGFB) signaling is disrupted in ME/CFS and plays a direct role in uncoupling central and peripheral circadian rhythms. R
Serum from ME/CFS patients causes loss of rhythm robustness in cellular circadian reporters, and recombinant Transforming Growth Factor Beta 1 (TGFB1) reduces rhythm amplitude and causes phase delay. R
This desynchronization means the body cannot properly time repair processes, mitochondrial biogenesis, and antioxidant enzyme production to the recovery window after exertion. R
Jacob frames this as a core mechanism of PEM: the circadian system that should coordinate recovery is itself broken, so each exertion event creates damage that accumulates rather than resolves.
The Kynurenine Shunt
Chronic interferon signaling activates Indoleamine 2,3-Dioxygenase (IDO1), which shunts tryptophan away from serotonin and melatonin synthesis and into the kynurenine pathway.
This produces Kynurenine (KYN), Kynurenic Acid (KYNA), and Quinolinic Acid (QUIN) at the expense of serotonin, melatonin, and NAD. R
Lower serotonin means vagal tone drops, pushing the autonomic nervous system into sympathetic dominance and making post-exertion recovery harder. R
Lower melatonin disrupts sleep quality, further degrading the recovery window.
The IDO metabolic trap hypothesis proposes that once tryptophan metabolism shifts into the kynurenine pathway past a critical threshold, it becomes bistable and cannot spontaneously return to normal without an exogenous perturbation. R
This is covered in depth in the Tryptophan, NAD, Kynurenine, Quinolinic, Serotonin, Vagus Nerve JD chapter.
The Energy Envelope Model
The Energy Envelope Model was developed by Leonard Jason and colleagues as a framework for understanding energy management in ME/CFS.
The model proposes that each person has a finite amount of available energy and that staying within that envelope, matching energy expenditure to available energy, prevents PEM and allows gradual functional improvement. R
Research consistently shows that patients who maintain energy envelope adherence experience less fatigue, better physical functioning, and fewer symptom exacerbations than those who regularly overextend. R
Overextending on a given day does not create a net gain in productivity.
It creates a debt that typically costs several days to several weeks of severely reduced capacity to repay. R
The Energy Quotient
I ask patients to rate their perceived available energy and their perceived expended energy each day on a 0 to 100 scale.
The energy quotient is (expended / available) x 100.
A score of 100 means perfect balance.
Scores above 120 indicate overextension and predict worse functioning and more severe PEM. R
I recommend keeping the daily quotient below 110 whenever possible.
This is not about doing less.
It is about doing only what the current energy envelope allows and nothing more.
The Activity Bank
Think of energy as a bank account with a very limited balance each day.
There are deposits (rest, sleep, pacing breaks, nutrition, vagal activation) and withdrawals (physical exertion, cognitive work, emotional stress, social interaction, environmental exposures).
The goal is not to zero out the account each day.
The goal is to leave a reserve so the next day opens with a positive balance.
Most ME/CFS patients live in chronic energy debt because they overdraw the account daily and never get a full night of repair. R
Practical Pacing Strategies
1. Find Your Baseline
Stop all non-essential activity for 3 to 7 days and observe what your body can do without triggering PEM.
Document the activities you can complete without a crash, the duration of each, and the recovery time needed afterward.
This baseline is lower than you think it is, and accepting that is the hardest part.
Patients who skip this step and start pacing from their current overextended state almost always fail because they never experience what non-crash days feel like. R
2. Use Heart Rate Monitoring
The Ventilatory Anaerobic Threshold (VAT) is the point at which your body switches from aerobic to anaerobic metabolism.
For healthy people, this happens at 60 to 80 percent of maximum heart rate.
For ME/CFS patients, the VAT can be as low as 40 to 50 percent of predicted max or even lower. R
Below the VAT, activity is sustainable and recovery is possible.
Above the VAT, lactate accumulates, mitochondrial stress increases, and PEM becomes likely.
Heart rate monitoring provides real-time feedback on whether you are above or below this threshold.
The practical rule is to stay at least 15 to 20 beats below your VAT heart rate for all activities.
Pacing with a heart rate monitor reduces PEM severity and duration, increases activity tolerance over time, and is rated as highly beneficial by 89 percent of users in survey research. R
I recommend a chest strap monitor for accuracy.
Wrist-based optical sensors are less reliable, especially during movement.
Set the upper alarm limit to your calculated pacing heart rate and stop or rest when the alarm sounds.
3. Activity Banking
Divide tasks into small, discrete chunks that fit within your energy window.
Never complete a task in one session if it can be broken into two or three smaller sessions with rests between.
I call this "activity banking" because each small deposit of effort must be matched by a deposit of rest.
The rule is one part activity, one part recovery.
If you walk for 5 minutes, rest for 5 minutes before the next activity.
If you read for 10 minutes, close your eyes for 10 minutes.
This ratio sounds extreme to people who have never experienced PEM.
For patients who can function on 15 minutes of activity per hour, it is liberating because it allows them to do more total over the course of a day without crashing.
4. Cognitive Pacing
Cognitive exertion triggers PEM just as reliably as physical exertion.
Concentrated reading, screen time, social interaction, decision making, and emotional processing all draw from the same energy account.
Use the same pacing rules for mental tasks.
Set a timer for focused cognitive work and take mandatory breaks equal to or longer than the work period.
Brown noise, blue blocker glasses, and reducing visual clutter can extend cognitive endurance.
5. Plan The Recovery Day
Assume that any day with above-baseline exertion, whether planned or unavoidable, requires a recovery day afterward.
Schedule recovery days proactively.
Do not wait until you crash to rest because by then the damage is done.
A recovery day means horizontal rest in a dark, quiet room, minimal cognitive input, no social demands, and frequent small meals.
This is not optional.
6. Learn Your Prodrome
Most patients have a recognizable set of early warning signs that a crash is coming.
These can include sore throat, tender lymph nodes, body temperature dysregulation, increased thirst, heavy limbs, visual changes, irritability, or word-finding difficulty.
Learn your specific prodrome and treat it as a non-negotiable stop signal.
When the prodrome appears, cancel all non-essential activity and begin crash recovery immediately.
7. Set Activity Ceilings
Decide in advance what the maximum activity level for any given day will be and do not exceed it regardless of how you feel.
The temptation to "bank" a good day by doing extra is the most common cause of the boom-bust cycle.
A good day is not an opportunity to catch up on everything you missed during the crash.
A good day is an opportunity to practice staying within the envelope and building trust in the recovery process.

Pacing Tools And Tracking
Heart Rate Monitors
A chest strap monitor like the Polar H10 or Garmin HRM-Pro provides accurate, real-time heart rate data.
Use it alongside an app that allows you to set heart rate zone alarms.
The Visible app is specifically designed for ME/CFS pacing and includes symptom tracking, heart rate monitoring, and energy envelope calculations.
The 10-Minute Stand Test
Measure your heart rate response to standing as a proxy for autonomic strain.
Take your resting heart rate after 10 minutes supine, then stand and measure heart rate at 1, 3, 5, and 10 minutes.
A sustained increase of 30 beats per minute or more, or a heart rate that continues climbing rather than stabilizing, suggests that even upright posture is a significant energy drain. R
Symptom And Activity Log
Track daily: perceived available energy (0-100), perceived expended energy (0-100), worst symptom type and intensity, activity type and duration, heart rate during activities, sleep quality and duration, PEM episodes (trigger, onset delay, duration, severity).
After two to four weeks, patterns emerge that make pacing decisions obvious.
Heart Rate Variability
Heart Rate Variability (HRV) reflects the balance between sympathetic and parasympathetic nervous system activity.
Low HRV in the morning predicts higher PEM risk that day.
Monitoring HRV trends over time helps identify whether the overall recovery trajectory is improving or declining. R
Many smart watches and chest straps report HRV automatically, but overnight readings are more reliable than single-point measurements.
Crash Recovery Protocol
When you have overextended and the crash hits, the priority is damage control, not productivity.
Immediate (First 24 Hours)
Stop all activity immediately when you recognize the prodrome or crash has begun.
Lie flat in a dark, quiet room with minimal sensory input.
Hydrate with electrolytes, not just water, because PEM involves vascular dysregulation and electrolyte shifting.
Do not attempt to "think your way out" or push through.
This will only extend the crash duration.
Nutritional Support
Eat small, frequent meals that are easy to digest.
Prioritize protein and electrolytes over carbohydrates.
Consider sublingual B12 or methylated B complex for mitochondrial cofactor support.
Coenzyme Q10 (CoQ10) and Nicotinamide Riboside (NR) can support the electron transport chain during recovery. R
Sleep Support
Do not fight the increased sleep need during a crash.
The body is attempting to repair mitochondrial damage, clear inflammatory debris, and restore redox balance.
Melatonin at a low dose (0.3 to 1 mg) supports circadian resynchronization.
Higher doses can overshoot and worsen morning grogginess.
Autonomic Reset
Gentle vagal activation via slow, diaphragmatic breathing (4 seconds in, 6 seconds out) can help shift out of sympathetic dominance.
Neck cooling with a cold pack on the carotid arteries or face immersion in cold water (the mammalian dive reflex) can dampen the adrenaline surge that often accompanies a crash.
Return Protocol
Do not resume normal activity immediately when the crash lifts.
Extend recovery by at least one full day beyond when you feel "normal."
The feeling of recovery is often a false summit, and resuming activity too soon triggers a second, often worse, crash.
Ramp back up at 50 percent of your pre-crash baseline for the first week, regardless of how good you feel.
Overlapping Conditions
POTS And Vaso-Adaptive Disorders
Orthostatic intolerance dramatically worsens PEM because upright posture alone imposes an energy cost.
Jacob reframes Postural Orthostatic Tachycardia Syndrome (POTS) as a Vaso-Adaptive Disorder (VAD) or Adrenergic-Based Vaso-Adaptive Disorder (ABVAD), where TCLS at the microcapillary level causes intravascular hypovolemia that classical volume sensors do not detect.
This is covered in the Microcapillaries And Vascular POTS chapter.
Heart rate pacing and activity banking must account for the additional energy drain of being upright.
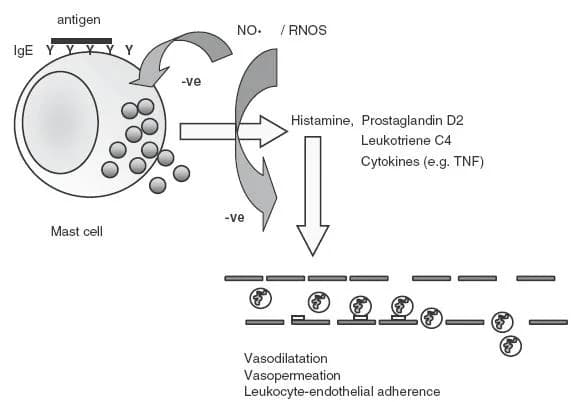
Mast Cell Activation
MCAS amplifies PEM through histamine-driven vasodilation, neurogenic inflammation, and TRP receptor sensitization. R
This is covered in Mast Cells, Substance P, And Neurogenic Inflammation.
Exertion triggers mast cell degranulation in susceptible individuals, adding a histamine-mediated inflammatory layer on top of the mitochondrial energy failure.
Small Fiber Neuropathy
Small Fiber Neuropathy (SFN) is prevalent in ME/CFS and causes autonomic dysfunction that impairs heart rate regulation, temperature control, and vascular tone. R
This is covered in my post on Small Fiber Neuropathy.
When the autonomic nervous system cannot properly regulate vascular tone, the heart must work harder to perfuse tissue during exertion, driving heart rate higher at lower workloads and making pacing with HR targets even more critical.
Histamine Intolerance
Histamine intolerance shares significant overlap with MCAS and impairs the vagal anti-inflammatory pathway.
This is covered in my comparison post on Histamine Intolerance Vs MCAS.
High-histamine foods can trigger symptom flares that mimic or amplify PEM, making dietary management relevant to energy stability.
CIRS
Chronic Inflammatory Response Syndrome overlaps with ME/CFS in approximately 30 percent of cases, but I reframe it through the junction dysfunction lens rather than the Shoemaker biotoxin model.
Both conditions share the same downstream pathology: glycocalyx damage, TCLS, MSS, immune paralysis, and impaired post-exertional recovery.
EDS And Hypermobility
Ehlers-Danlos Syndrome (EDS) and hypermobility spectrum disorders predict worse PEM because compromised connective tissue means reduced capillary reserve, impaired vascular tone, and greater vulnerability to mechanotransduction damage during exertion.
The collagen defects that make joints hypermobile also affect blood vessel integrity, compounding the energy delivery problem.
Testing
Cardiopulmonary Exercise Testing
Two-day CPET is the gold standard for objectively documenting PEM.
The Workwell Foundation and several academic centers offer this protocol.
A decrease in workload at ventilatory threshold of 6.3 to 9.8 percent on day two provides high sensitivity and specificity for distinguishing ME/CFS from controls. R
Heart Rate Variability And Autonomic Testing
I use the POTS bundle which includes the Cellular Zoomer for mitochondrial markers, Hormone Zoomer for adrenal and circadian assessment, Gut Zoomer for microbiome and permeability, and Neural Zoomer for autonomic and neurological markers.
The Neural Zoomer (Vibrant Wellness) assesses brain autoimmunity, blood-brain barrier integrity, demyelination, and peripheral neuropathy markers relevant to autonomic dysfunction.
Blood And Urine Markers
Lactate: elevated at rest or after minimal exertion suggests early anaerobic threshold and mitochondrial impairment. R
Included in the Cellular Zoomer.
ANGPT2: elevated levels correlate with glycocalyx degradation and endothelial dysfunction.
Available through research labs; not yet standard clinical.
TGFB1: elevated TGFB1 signaling is associated with circadian disruption and immune dysregulation in ME/CFS. R
Included on the Immune Zoomer.
Kynurenine pathway metabolites: elevated kynurenine/tryptophan ratio, reduced serotonin, altered 3-HK and QUIN levels indicate IDO activation.
These are assessed through the Cellular Zoomer and Organic Acids Test (OAT). R
CoQ10: low levels correlate with mitochondrial dysfunction and predict worse exercise tolerance. R
Assessed through the Cellular Zoomer and the Nutrient Zoomer.
Vitamin D: deficiency is common in ME/CFS and impairs mitochondrial function and immune regulation. R
Assessed through the Nutrient Zoomer.
Cortisol: multi-point saliva testing is preferred over single-point serum.
ME/CFS often presents with a flattened or inverted cortisol rhythm rather than the classic low or high pattern. R
Assessed through the Hormone Zoomer or a dedicated DUTCH Complete (Precision Analytical).
Functional Lab Panels
I use the Long COVID bundle to assess the full picture in patients with post-viral PEM.
It includes the Cardio Zoomer (endothelial function, lipid metabolism, insulin resistance), Toxin Zoomer (mycotoxins, heavy metals, environmental chemicals), Gut Zoomer, Cellular Zoomer, and Viral Infections Panel.
I use the General Wellness bundle for baseline assessment of energy systems, including the Foundation Zoomer (CBC, CMP, thyroid), Hormone Zoomer, Nutrient Zoomer, and Cellular Zoomer.
For redox and mitochondrial genetic assessment, I use the Cellular Zoomer which measures organic acids, mitochondrial function markers, and oxidative stress indicators.
Mechanisms Of Action
Simple:
PEM happens because cells cannot produce enough energy to meet the demand of activity and cannot repair the damage caused by the activity, so each exertion event creates a deficit that accumulates over time instead of resolving overnight.
Pacing keeps activity below the threshold where energy demand exceeds energy production capacity, allowing the repair systems to keep up with the damage.
Heart rate monitoring works because the ventilatory threshold, the point at which aerobic energy production can no longer keep up and anaerobic metabolism kicks in, is objectively measurable, and staying below it prevents the metabolic cascade that triggers PEM.
Advanced:
- Mitochondrial M1 State persistence: Macrophage mitochondria in ME/CFS remain in a pro-inflammatory, high-ROS state characterized by increased Reactive Oxygen Species (ROS) production, reduced Adenosine Triphosphate (ATP) yield, and impaired Electron Transport Chain (ETC) complex I and IV activity. WASF3 overexpression disrupts respiratory supercomplex formation, reducing complex IV assembly and creating a ceiling on oxidative phosphorylation capacity. R
- ANGPT2/TIE2 destabilization loop: Glycocalyx degradation reduces TIE2 phosphorylation and increases ANGPT2 release from endothelial cells. ANGPT2 antagonizes TIE2, promoting endothelial junction instability, microcapillary rarefaction, and impaired oxygen delivery to tissue. This raises the fraction of oxygen extraction required at any given workload, pushing the body past VAT earlier. R
- TGFB-driven circadian uncoupling: Elevated TGFB1 signaling desynchronizes peripheral circadian clocks from the central suprachiasmatic pacemaker. CLOCK and BMAL1 expression is phase-shifted in skeletal muscle and endothelial cells, so the timing of mitochondrial biogenesis, antioxidant enzyme production, and autophagy no longer aligns with the post-exertion recovery window. R
- IDO1/kynurenine shunt and vagal dysfunction: Interferon-gamma activates IDO1, depleting tryptophan available for serotonin synthesis. Reduced gut serotonin leads to loss of vagal parasympathetic tone, shifting autonomic balance to sympathetic dominance and impairing post-exertion parasympathetic recovery. KYNA antagonizes the alpha-7 nicotinic acetylcholine receptor on macrophages, blocking the vagal anti-inflammatory pathway. R
- Lactate clearance failure: In healthy individuals, lactate produced during exertion is cleared by the liver, heart, and skeletal muscle via the Cori cycle and monocarboxylate transporters. ME/CFS patients show impaired lactate clearance post-exertion, consistent with mitochondrial dysfunction and reduced MCT expression, prolonging the metabolic acidosis and inflammatory signaling that follows exertion. R
Genetics
WASF3
The WASF3 gene encodes a protein involved in cytoskeletal dynamics and mitochondrial supercomplex assembly.
Overexpression of WASF3 disrupts respiratory supercomplex formation and reduces complex IV activity in skeletal muscle mitochondria. R
No single common variant has been linked to elevated WASF3 expression, but ER stress inducers, including endotoxin and inflammatory cytokines, upregulate WASF3 transcription significantly.
rs55724298: variant in the WASF3 regulatory region associated with altered expression levels in response to inflammatory stress (preliminary data).
SOD2
SOD2 encodes manganese superoxide dismutase, the primary mitochondrial antioxidant enzyme that sits on the glycocalyx surface.
rs4880: Ala16Val substitution reduces SOD2 import into mitochondria by 30 to 40 percent, impairing superoxide quenching capacity and increasing vulnerability to exercise-induced oxidative damage. R
This is in Jacob's priority SNP list and is one of the most common variants in his client population.
IDO2
The IDO2 gene encodes a tryptophan-degrading enzyme paralogous to IDO1, but with much lower catalytic activity.
Four common damaging mutations in IDO2 render it non-functional in a significant portion of the population. R
Non-functional IDO2 combined with substrate inhibition of IDO1 creates the conditions for the IDO metabolic trap, a bistable switch in tryptophan metabolism that may explain why PEM persists indefinitely once established. R
rs4503083: loss-of-function variant in IDO2 that reduces kynurenine pathway capacity and increases susceptibility to the metabolic trap (preliminary data).
IFITM3
IFITM3 encodes interferon-induced transmembrane protein 3, which restricts viral entry.
rs12252: the CC genotype is associated with severe COVID-19 and may predict higher risk of post-viral ME/CFS onset. R
ACE2
ACE2 is the entry receptor for SARS-CoV-2 and a key regulator of the renin-angiotensin system.
Lower ACE2 expression or activity reduces the conversion of Angiotensin II to Angiotensin 1-7, shifting toward vasoconstrictive, pro-inflammatory signaling that impairs exercise tolerance and recovery. R
rs2285666: variant associated with reduced ACE2 expression, linked to higher risk of severe COVID-19 and potentially worse post-viral PEM.
More Research
- Activity pacing versus graded exercise in trials: A 2023 scoping review of pacing in ME/CFS concluded that pacing is the most commonly reported coping strategy among patients but remains understudied in controlled trials, with most evidence coming from observational and survey-based designs. Definitive RCTs using objective activity monitoring are needed. R
- Conflicting evidence on two-day CPET reliability: A 2026 study by Mancini et al. found no significant day-two decline in peak VO2 or VO2 at ventilatory threshold in 58 ME/CFS patients, contradicting the larger 2024 Keller study. The authors suggest that subjective symptom monitoring after exercise may be a more sensitive marker of PEM than CPET metrics alone. This highlights that no single objective test is sufficient for PEM assessment.
- Plasma metabolomics of exercise recovery: A 2022 JCI Insight study tracked 1,157 plasma metabolites across two-day CPET in 60 ME/CFS patients and 45 controls. Lipid metabolism, energy pathways, the malate-aspartate shuttle, and the glucose-alanine cycle were all disrupted in patients during the 24-hour recovery period. Over a quarter of identified pathways remained significantly different from controls after the recovery window. R
- Glutamate metabolism and brain energy: The same metabolomics study identified glutamate metabolism as a central hub of dysregulation during recovery. Glutamate is crucial for brain energy homeostasis, and its disruption may explain the cognitive PEM component that patients describe as "brain fog."
- For biomarker testing I use the Cellular Zoomer to assess mitochondrial function, the Hormone Zoomer for adrenal and circadian rhythm assessment, and the Long COVID bundle for comprehensive post-viral evaluation.
- For genetics, I use the Methylation Genetics panel for methylation cycle SNPs and the Cellular Zoomer for oxidative stress markers, alongside raw 23andMe data analyzed against Jacob's priority SNP list from the JD genetics chapter.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Lion's Mane
1000mg/day
Omega-3 (DHA)
2g/day
Phosphatidylserine
100mg 3x/day