Coregulation, Nervous System Dysregulation, And PTSD
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Post-traumatic stress disorder (PTSD) is fundamentally a disorder of autonomic dysregulation in which the nervous system becomes locked in defensive states, loses access to the circuitry that allows social connection to calm the body, and misidentifies ordinary environments as threatening, independent of what the conscious mind knows.
In this post, we will discuss what coregulation is and why it is biologically necessary, how the autonomic nervous system is organized, what PTSD does to that organization at a measurable physiological level, how faulty threat detection drives the symptom picture, which conditions overlap with this dysregulation pattern, what you can do to restore autonomic flexibility, what to avoid, the underlying mechanisms, and the genetics.
Basics: The Autonomic Nervous System And Its Hierarchy
The autonomic nervous system (ANS) controls involuntary physiology: heart rate, respiration, digestion, immune function, and the moment-to-moment calibration of threat versus safety.
It is not a simple on-off switch between calm and stress.
It is a hierarchically organized system shaped by vertebrate evolution, and understanding that hierarchy is the entry point for understanding both PTSD and coregulation. R
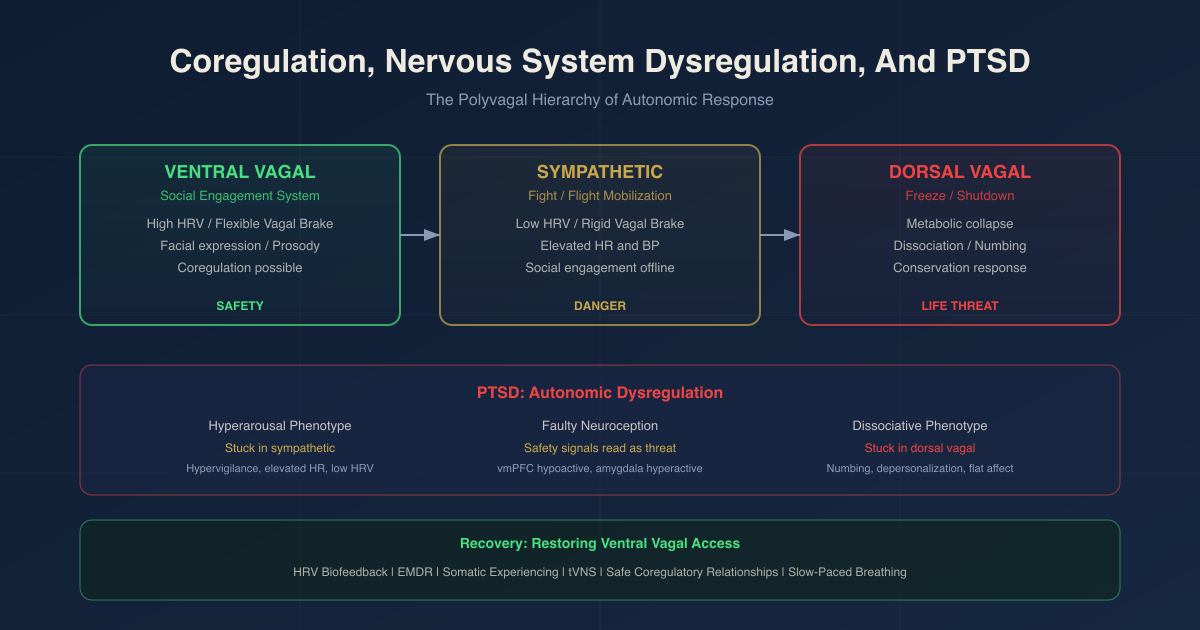
Polyvagal Theory, developed by Stephen Porges, PhD, proposes a three-tier phylogenetic hierarchy of autonomic response strategies: R
Tier 1: Ventral Vagal (Social Engagement)
This is the newest system, unique to mammals.
The ventral vagal complex (VVC) involves myelinated vagal pathways originating in the nucleus ambiguus in the brainstem.
The VVC connects cardiac regulation to the muscles of the face and head (middle ear, larynx, pharynx, facial expression, eye gaze) through what Porges calls the social engagement system. R
When this system is active:
The heart rate slows and becomes flexible.
The face becomes expressive and readable.
The voice acquires prosody (warmth and rhythm).
The middle ear muscles tune to the frequency range of the human voice.
Digestion, tissue repair, and immune homeostasis are all supported. R
This is the state in which coregulation is possible.
Safety is communicated through the face and voice, and the nervous system of another person can receive those signals and be calmed by them.
Tier 2: Sympathetic Activation (Mobilization)
When the VVC is withdrawn, the sympathetic nervous system (SNS) takes over.
Heart rate increases.
Pupils dilate.
Blood redirects to large muscle groups.
Breathing becomes shallow and rapid.
The body prepares for fight or flight.
Social engagement becomes functionally impossible: the middle ear muscles relax and the voice of another person becomes noise rather than signal. R
Tier 3: Dorsal Vagal (Immobilization)
If mobilization does not resolve the threat, an older system takes over.
Dorsal vagal pathways originating in the dorsal motor nucleus of the vagus (DMNX), shared with reptiles, drive a conservation/shutdown response.
Heart rate drops dramatically.
Metabolic rate falls.
The person may freeze, dissociate, collapse, or feign death.
This is the physiological substrate of the numbing and dissociation seen in complex PTSD and freeze responses. R
The hierarchy operates in a specific order.
The VVC is the first to be recruited.
If it fails to resolve the perceived threat, the SNS activates.
If sympathetic mobilization fails, the dorsal vagal shutdown activates.
These circuits do not simply alternate.
They can be recruited simultaneously, producing the "freeze with fear" hybrid state: high sympathetic tone (vigilant, scanning, heart pounding) combined with dorsal vagal immobility (unable to move or speak). R
The vagal brake is the myelinated VVC's ability to rapidly inhibit or release sympathetic influence on the heart.
A flexible vagal brake allows rapid adjustment between calm and mobilized states and rapid recovery back to calm.
A rigid or collapsed vagal brake keeps the nervous system stuck. R
Heart rate variability (HRV) is the primary measurable biomarker of VVC tone and vagal brake function.
Respiratory sinus arrhythmia (RSA), the rhythmic increase in heart rate during inhalation and decrease during exhalation, is the non-invasive index of myelinated vagal activity and autonomic flexibility. R
What Coregulation Is And Why It Matters
Coregulation is the process through which one nervous system stabilizes another's autonomic state through interpersonal cues of safety.
It operates at hormonal (cortisol, oxytocin), autonomic (HRV, RSA), and central nervous system (neural attunement, brain-to-brain coupling) levels simultaneously. R
It is not a psychological metaphor.
It is a measurable, cross-species biological phenomenon in which autonomic states synchronize bidirectionally between individuals in proximity. R
Coregulation predates self-regulation.
Human infants cannot self-regulate.
Their nervous systems are too immature.
Self-regulation capacity develops only through repeated coregulatory experiences with a regulated caregiver. R
Each time a caregiver's calm face, steady voice, and rhythmic touch bring an infant from distress to calm, neural circuits are being sculpted.
The infant's nervous system is learning the pattern: distress can resolve, other nervous systems are trustworthy, and social engagement produces calm. R
When this developmental scaffolding is disrupted by neglect, abuse, loss of caregiver, or chronic unpredictability, the nervous system never learns that the social engagement system is a reliable route to safety.
It defaults to defensive strategies. R
Coregulation in adults.
Adults continue to coregulate throughout life, though the contribution of self-regulation increases.
Social support is one of the most consistent protective factors against PTSD after trauma exposure, and its protective effect is not primarily cognitive.
It is autonomic.
A regulated nervous system in proximity communicates safety to an unregulated one through prosody, facial expression, and physical proximity. R
The channels through which coregulation operates include:
- Vocal prosody (warmth, rhythm, pace of speech)
- Facial expression (especially periorbital muscle tone and eyebrow position)
- Touch (particularly slow, rhythmic, non-threatening contact)
- Breathing synchrony (matched breathing rhythms between individuals)
- Eye contact (safe and regulated, not fixed or threatening)
These are the features of the social engagement system.
Each of them is neurally linked to VVC activity in both the sender and the receiver. R
The coregulation paradox in PTSD:
PTSD disrupts access to the very mechanism needed for recovery.
People with PTSD have downregulated social engagement systems.
Their neuroception (the ANS's threat-detection system, discussed below) identifies social proximity as threatening rather than soothing.
The faces, voices, and touch of other people, which are the primary inputs to coregulation, trigger defensive rather than social engagement responses.
The system that should heal has been functionally blocked by the condition itself. R
What Trauma Does To The Nervous System
PTSD is a condition of autonomic dysregulation, not just a memory or cognitive disorder.
A meta-analysis of HRV studies in PTSD found that individuals with PTSD have lower HRV than healthy controls both at rest and during stress, with reduced parasympathetic (vagal) activity reflected across multiple indices: RMSSD (root mean square of successive differences), HF-HRV (high-frequency power), and SDNN (standard deviation of NN intervals). R
The LF/HF ratio is elevated in PTSD compared to controls, consistent with a shift toward sympathetic dominance and a reduction in sympatho-vagal balance. R
Elevated resting heart rate and systolic blood pressure are found in PTSD, driven by increased central and peripheral sympathetic activity and elevated noradrenergic tone originating from the locus coeruleus. R
What this means clinically:
Reduced HRV means the vagal brake is rigid.
The person cannot efficiently shift between states.
They cannot move from hyperarousal back to calm.
They cannot engage the social engagement system reliably.
They are metabolically expensive to maintain: a chronically activated sympathetic nervous system drives sustained cortisol secretion, elevated inflammatory cytokines, and increased cardiovascular workload. R
The adrenal output is paradoxically low in PTSD.
Unlike depression, which is associated with elevated cortisol, PTSD is typically associated with low cortisol alongside elevated CRH and high glucocorticoid receptor (GR) sensitivity.
The HPA axis has become hypersensitive to negative feedback: even low cortisol levels adequately suppress CRH output.
Low cortisol fails to restrain inflammation, which then acts as a chronic stressor and perpetuates HPA dysfunction in a self-reinforcing loop. R
The two PTSD autonomic phenotypes:
The hyperarousal phenotype: persistent sympathetic activation, heightened startle, hypervigilance, reduced HRV, elevated HR.
The dissociative phenotype: dorsal vagal dominance, emotional numbing, derealization, depersonalization, apparent calm on the surface with physiological flattening underneath.
Both represent the ANS stuck in a defensive mode, but at different tiers of the polyvagal hierarchy. R
The hyperaroused person cannot come down.
The dissociated person cannot come up.
Both have lost autonomic flexibility.
PTSD and cardiovascular risk:
The persistent sympathetic hyperactivity in PTSD is an independent predictor of negative cardiovascular outcomes.
People with PTSD have significantly elevated risks of cardiovascular disease, hypertension, myocardial infarction, and all-cause mortality, driven by chronic autonomic imbalance, HPA axis dysregulation, endothelial dysfunction, and chronic inflammation. R
This is not an abstract risk.
Autonomic dysregulation in PTSD is a systemic physiological condition with measurable downstream organ consequences.
Neuroception: Why The Nervous System Misreads Safety In PTSD
Neuroception is Stephen Porges' term for the process by which the nervous system evaluates risk in the environment and assigns an autonomic state response, without conscious awareness. R
It is not perception in the cognitive sense.
It is a subcortical, pre-conscious threat assessment that fires before the cortex has processed the information.
Neural structures involved in neuroception include areas of the temporal cortex that decode biological movement and detect intentionality in social interactions, the amygdala (which responds to subliminal threat cues before conscious awareness), and the periaqueductal gray. R
Subliminal fear cues (faces shown too briefly to be consciously perceived) activate the superior colliculus, locus coeruleus, and amygdala in healthy individuals.
In PTSD, this innate alarm system is overactivated: the magnitude of amygdala response to subliminal threat cues is increased, and the system fires more readily and for longer. R
Faulty neuroception in PTSD:
The autonomic nervous system of a person with PTSD has been recalibrated by trauma to assign threat to stimuli that a healthy nervous system would register as safe. R
A raised voice, a sudden movement, a neutral facial expression, physical closeness, or even a change in ambient sound can trigger sympathetic activation or dorsal vagal shutdown before the prefrontal cortex has time to evaluate whether the stimulus is actually dangerous.
This is not a cognitive error.
It is a recalibrated autonomic set-point.
The nervous system is doing exactly what it was shaped to do.
It is responding accurately to its own internal threat model.
The problem is that the threat model was built in conditions that no longer apply. R
The vmPFC failure:
The ventromedial prefrontal cortex (vmPFC) is the brain structure most responsible for top-down inhibition of amygdala threat responses.
It learns through extinction: if a conditioned threat cue is repeatedly experienced without the original threat, the vmPFC develops inhibitory connections to the amygdala that suppress the fear response. R
PTSD is associated with vmPFC hypoactivity.
Decreased vmPFC activation to trauma-related cues is one of the most replicated neuroimaging findings in PTSD and corresponds to the failure of extinction learning that drives symptom persistence. R
The amygdala is not the problem.
The problem is that the brake on the amygdala is not functioning adequately.
Treatments that work (EMDR, prolonged exposure, successful pharmacotherapy) are associated with restored vmPFC activation and connectivity. R
The consequence for coregulation:
When neuroception is misfiring, the social engagement system cannot come online.
Faces that are offering safety are registered as threatening.
Voices that are calm are evaluated as dangerous.
The physiological substrate for receiving coregulation has been blocked at the subcortical level, below the reach of cognitive reassurance. R
This is why telling someone with PTSD to "just relax" or "you're safe now" accomplishes nothing physiologically.
The cognitive layer knows.
The autonomic layer does not. R
Overlapping Conditions
Developmental Trauma And Complex PTSD (C-PTSD)
When trauma occurs in developmental periods rather than isolated adult events, the disruption of coregulation is foundational rather than superimposed on an already-developed regulatory system.
Children raised without consistent, regulated caregivers develop nervous systems calibrated to chronic threat.
The VVC is systematically underdeveloped.
The sympathetic and dorsal vagal circuits dominate.
What later looks like personality pathology, affect dysregulation, identity disturbance, and chronic shame is in many cases the behavioral expression of an autonomic nervous system that never had its regulatory architecture properly built. R
Fibromyalgia And Chronic Pain
Fibromyalgia shares the autonomic signature of PTSD: reduced HRV, sympathetic dominance, blunted HPA feedback, and a central sensitization that resembles the amygdala hyperreactivity of trauma. R
The overlap is not coincidental.
Fibromyalgia has high rates of childhood adversity and trauma history, and the nervous system's chronic defensive posture drives the central sensitization that amplifies pain signals. R
POTS And Dysautonomia
Autonomic dysregulation in PTSD directly overlaps with the dysautonomia picture.
Reduced baroreflex sensitivity, impaired heart rate recovery, sympathetic hyperactivation at rest, and orthostatic intolerance share neurophysiological mechanisms with the HRV abnormalities of PTSD.
Many patients with POTS have significant trauma histories, and the two conditions may share common autonomic dysregulation pathways rather than being coincident comorbidities.
Irritable Bowel Syndrome And Gut Dysmotility
The vagus nerve is the primary communication highway between the gut and brain.
VVC hypofunction reduces parasympathetic tone to the gut, impairing motility, gut barrier function, and the anti-inflammatory cholinergic reflex that the vagus normally provides.
Gut dysbiosis and increased intestinal permeability are associated with PTSD and may be partially mediated by reduced vagal tone. R
Autoimmune And Inflammatory Conditions
Reduced VVC activity withdraws the cholinergic anti-inflammatory pathway from the periphery.
The vagus normally releases acetylcholine at target organs, suppressing macrophage activation and pro-inflammatory cytokine production (TNF-alpha, IL-1-beta, IL-6).
When vagal tone is chronically low, this anti-inflammatory brake is removed, and systemic inflammation increases. R
PTSD is associated with elevated inflammatory markers and increased rates of autoimmune disease. R
How To Restore Autonomic Regulation
The sequence matters here.
The nervous system has to feel safe enough to receive the inputs that restore safety.
A chronically dysregulated nervous system cannot simply decide to regulate.
It needs repetitive, biologically credible safety signals before the VVC comes back online.
The intervention categories below are ordered from those that bypass the need for felt safety (bottom-up) to those that require some VVC access to be effective (top-down).
1. HRV Biofeedback
HRV biofeedback (HRVB) trains slow-paced breathing (typically 4.5 to 6 breaths per minute, individualized to the person's resonance frequency) while providing real-time feedback on heart rate oscillations.
This pacing engages the baroreflex (the pressure-sensing feedback loop between the heart and brainstem) and maximally amplifies RSA, directly exercising the vagal pathway. R
A meta-analysis of HRV biofeedback across military PTSD populations found a moderate to large mean effect for PTSD symptom reduction (Hedges' g = -0.557, P < 0.001), with a cumulative attrition rate of only 5.8%, significantly lower than traditional PTSD therapies. R
A randomized waitlist-controlled trial of 6 weeks of HRVB in adults with co-occurring PTSD and chronic pain found a 24.3% reduction in PTSD checklist scores (d = -1.89), an 18.9% reduction in trauma-related distress, and a 24.9% improvement in pain interference. R
HRV biofeedback modulates HPA axis activity, reducing cortisol secretion and enhancing parasympathetic outflow.
It also strengthens prefrontal cortex connectivity with autonomic brainstem centers, supporting the vmPFC function that is deficient in PTSD. R
Practical: Resonance frequency breathing at approximately 5 to 6 breaths per minute.
This corresponds to an inhale of about 5 seconds and an exhale of about 5 to 6 seconds.
The extended exhale specifically activates the vagal brake.
20 minutes daily is the standard protocol in most studies.
A HRV biofeedback device provides real-time feedback to optimize breathing pattern.
2. Slow-Paced Breathing And Extended Exhale
Even without biofeedback hardware, slow diaphragmatic breathing with an extended exhale directly stimulates vagal afferents and increases RSA.
The critical ratio: exhale should be equal to or longer than inhale.
A 4-count inhale and 6-count exhale is a reasonable starting point. R
Paced breathing that achieves resonance frequency (approximately 0.1 Hz heart rate oscillations) produces the largest RSA amplitude and the greatest vagal engagement. R
3. EMDR (Eye Movement Desensitization And Reprocessing)
EMDR is a first-line treatment for PTSD with the strongest evidence base.
Twenty-four randomized controlled trials support its effectiveness for emotional trauma and adverse life experiences.
Seven of ten studies found EMDR more rapid or more effective than trauma-focused CBT. R
EMDR produces measurable autonomic changes during sessions.
At the onset of bilateral stimulation sets, a sharp increase in HRV and significant decrease in heart rate occurs (de-arousal).
Across entire sessions, progressive decreasing HR and increasing HRV demonstrates a cumulative autonomic calming effect. R
The Adaptive Information Processing (AIP) model underlying EMDR proposes that traumatic memories are stored in a state-dependent, isolated network that preserves the original sensory and somatic experience.
EMDR reprocesses this network through dual attention (bilateral stimulation while holding the traumatic memory), allowing information to integrate into the broader adaptive memory network.
The autonomic signature of this integration is increased HRV and reduced sympathetic activation across sessions. R
4. Somatic Experiencing
Somatic Experiencing (SE) is a body-oriented therapy developed by Peter Levine that works directly with the incomplete defensive responses stored in the nervous system.
In SE, the therapist helps the client track sensations (rather than narratives), pendulate between resource states and trauma activation, and allow incomplete survival responses to complete.
A scoping literature review found preliminary evidence for positive effects of SE on PTSD-related symptoms, affective symptoms, somatic symptoms, and well-being, with practitioners identifying resource-orientation and the titration of trauma activation as method-specific key factors. R
SE works through the body-up rather than top-down, which is important for people whose trauma is pre-verbal, pre-narrative, or whose nervous systems are too dysregulated to access cognitive processing.
5. Coregulation Through Therapeutic Relationships
The therapeutic relationship itself is a coregulatory device when the therapist maintains a regulated state.
The therapist's prosodic voice, calm facial expression, measured physical proximity, and paced breathing all transmit cues of safety to the client's autonomic nervous system through the social engagement system. R
This is why the modality of trauma therapy is often secondary to the quality of the therapeutic alliance.
A dysregulated therapist, regardless of technique, cannot coregulate a dysregulated client. R
6. Safe Pets, Animals, And Regulated Social Contact
Animal-assisted contact (pets, therapy animals) provides a coregulatory input without the complexity of human social threat processing.
Animals signal safety through different channels than humans.
For people whose neuroception misidentifies human faces and voices as threatening, contact with a regulated animal may be a more accessible entry point to the VVC. R
The same principle applies to finding reliably regulated people: friends, family members, or support group members whose presence consistently produces felt safety.
Oxytocin, released during safe affiliative contact, acts at the amygdala to reduce fear-potentiated startle and facilitates access to the social engagement system. R
7. Transcutaneous Vagal Nerve Stimulation (tVNS)
Non-invasive transcutaneous vagal nerve stimulation (tVNS) delivers electrical stimulation to the auricular branch of the vagus nerve at the ear.
A clinical trial found that repeated tVNS administration in PTSD patients (compared to sham) produced accrued reductions in heart rate over time, with effects selectively present in the PTSD group rather than the non-PTSD trauma-exposed group, consistent with targeting pathological pathways specific to PTSD.
Results suggest long-term autonomic recalibration with chronic use. R
tVNS devices are increasingly available for consumer use.
A tVNS auricular device provides accessible non-invasive vagal stimulation outside clinical settings.
8. Exercise (Graded And Non-Triggering)
Aerobic exercise increases HRV and vagal tone when not performed at a level that triggers trauma-associated sympathetic hyperarousal.
The key is not intensity.
It is predictability, a sense of autonomy over the experience, and the absence of sudden unexpected stimuli that might trigger the innate alarm system.
Rhythmic, low-novelty exercise (walking, swimming, cycling) at moderate intensity is better tolerated than high-intensity interval training for people with PTSD who have significant autonomic dysregulation.
9. Phosphatidylserine For HPA Axis Normalization
Phosphatidylserine (PS) normalizes the hyper-responsivity of the HPA axis to acute stressors in chronically stressed individuals.
400 mg PS + 400 mg phosphatidic acid (PAS 400) for 3 weeks significantly normalized ACTH (p = 0.010) and cortisol (p = 0.035) responses to psychosocial stressors, with selective effects in high-stress subjects. R
In individuals with blunted cortisol response at baseline (the PTSD-type low cortisol phenotype), omega-3-enriched phosphatidylserine appeared to restore (increase) the blunted cortisol response toward normal, demonstrating a bidirectional normalizing effect. R
Typical dosing: 400 to 800 mg daily.
10. Magnesium For Sympathetic Braking
Magnesium glycinate acts as a natural NMDA receptor antagonist and reduces noradrenergic transmission.
Chronic stress depletes magnesium, and magnesium deficiency exacerbates sympathetic hyperactivation and startle responses.
Supplementation does not directly restore VVC tone but reduces the sympathetic substrate that competes with parasympathetic activation.
Typical dosing: 300 to 400 mg elemental magnesium at night.
What To Stay Away From
- Chronic alcohol use, which mimics GABAergic sedation acutely but produces rebound sympathetic hyperactivation and reduced HRV chronically, and is strongly associated with HPA axis uncoupling (blunted ACTH and adrenal hypertrophy) that mirrors the PTSD dysregulation pattern R
- Chronic cannabis use, which acutely reduces sympathetic activation but chronically reduces HRV and blunts autonomic responsiveness, impairing the flexibility that is already deficient in PTSD
- Chronic sleep restriction, which keeps the SNS activated and prevents the HRV and autonomic recovery that occurs predominantly during deep and REM sleep R
- Social isolation, which removes the primary biological input for coregulation and allows defensive autonomic states to consolidate without correction R
- Chronic exposure to dysregulated or threatening social environments (abusive relationships, high-conflict households, chaotic workplaces), which continue to drive faulty neuroception recalibration and prevent VVC access R
- High-dose caffeine, particularly in the afternoon and evening, which extends sympathetic activation into the recovery window and suppresses the parasympathetic predominance of evening and nighttime
- Overtraining without recovery, which chronically elevates sympathetic tone and cortisol and reduces HRV in the same way chronic psychological stress does R
- Unpredictable or sudden sensory environments, including loud, chaotic, or visually overwhelming spaces, which load the innate alarm system and prevent the nervous system from sustaining the ventral vagal state long enough to consolidate regulation R
Mechanisms Of Action
Simple:
- Trauma recalibrates the autonomic nervous system to assign a defensive set-point, shifting it away from ventral vagal flexibility and toward chronic sympathetic hyperactivation or dorsal vagal shutdown R
- The social engagement system (face, voice, middle ear, VVC) becomes functionally blocked, so people with PTSD cannot receive or transmit the cues of safety needed for coregulation R
- The innate alarm system becomes hypersensitive: subliminal threat cues (faces, sounds, body postures) that healthy nervous systems process below threshold are enough to trigger full amygdala activation and sympathetic mobilization in PTSD R
- The vmPFC, which normally inhibits the amygdala through extinction learning, is hypoactive in PTSD, so conditioned fear responses cannot be adequately suppressed R
- HRV is reduced because the vagal brake is rigid: the VVC cannot rapidly modulate cardiac output in response to contextual demands R
- HRV biofeedback, slow breathing, and therapeutic coregulation all work by repeatedly activating the RSA/baroreflex pathway, exercising the myelinated vagal circuit and gradually restoring its flexibility R
Advanced:
The vagal paradox and the two vagal systems:
The unmyelinated dorsal vagal pathways (originating in the DMNX) existed in early vertebrates.
They produce the reptilian freeze and death-feign response.
When combined with sympathetic tone, they produce the freeze-with-fear state. R
The myelinated ventral vagal pathways (originating in the nucleus ambiguus) are evolutionarily derived and uniquely mammalian.
They produce the rapid, rhythmic heart rate modulation that constitutes RSA.
They connect cardioinhibitory function to the facial and vocal musculature through cranial nerves V (trigeminal), VII (facial), IX (glossopharyngeal), X (vagus), and XI (accessory), forming the social engagement system. R
The face-heart connection is not metaphorical.
The same brainstem nucleus (nucleus ambiguus) that regulates heart rate also regulates laryngeal and pharyngeal muscles.
When you hear a safe voice, the cardiac rhythm is directly modulated by the same brainstem circuit that is processing the vocal prosody. R
This is why music with vocal elements, certain frequencies of human voice, and prosodic speech have direct autonomic effects that pure noise does not. R
Neuroception and the innate alarm system:
The innate alarm system (IAS) is a network of midbrain and brainstem nuclei (superior colliculus, locus coeruleus, periaqueductal gray) that detects and transmits threat signals below the level of cortical awareness.
Subliminal fearful faces activate this network, generating amygdala responses before conscious processing, through a thalamo-amygdala pathway that bypasses primary visual cortex. R
In PTSD, the IAS is tonically sensitized.
The superior colliculus and locus coeruleus show increased activation in response to subliminal threat, the periaqueductal gray shows increased resting-state functional connectivity with emotional reactivity areas, and the amygdala startle threshold is reduced. R
This sensitization operates below conscious control and cannot be addressed by cognitive therapy alone.
It requires inputs that recalibrate the subcortical threat-detection system directly, which is why bottom-up approaches (HRV biofeedback, somatic therapies, vagal stimulation) are often needed to create the autonomic stability from which cognitive processing can then be effective. R
The cholinergic anti-inflammatory pathway:
Vagal efferents to the spleen, liver, and gut release acetylcholine at target macrophages.
Acetylcholine binding to alpha-7 nicotinic receptors on macrophages suppresses TNF-alpha and IL-1-beta production.
When vagal tone is chronically reduced, this brake on peripheral inflammation is removed.
The resulting elevated inflammatory cytokines cross back into the brain and further dysregulate limbic threat circuits, creating a bidirectional inflammatory-autonomic loop that perpetuates PTSD. R
HRV biofeedback and vagal stimulation restore this cholinergic anti-inflammatory pathway, which partially explains why vagal tone improvements in PTSD are accompanied by reductions in inflammatory markers. R
Oxytocin and the social engagement system:
Oxytocin is synthesized in the paraventricular and supraoptic nuclei of the hypothalamus and projects centrally to the amygdala, hippocampus, nucleus accumbens, and anterior cingulate cortex.
It dampens amygdala reactivity to threat cues and reduces fear-potentiated startle.
Lack of social support is one of the most consistent risk factors for PTSD, and the oxytocin system has been proposed as a primary mediator of social support's protective effects. R
Intranasal oxytocin administration in PTSD patients dampens amygdala reactivity to emotional faces in both males and females.
It improves empathic accuracy and reduces conditioned fear responses.
The effects are most pronounced in individuals with early trauma and lower baseline social attachment. R
Endogenous oxytocin release during safe affiliative contact (touch, prosodic voice, eye contact, coregulation with a trusted person) represents the physiological mechanism through which human connection directly modulates PTSD symptomatology at the amygdala level. R
Genetics
OXTR (oxytocin receptor gene) variants:
Variants in the oxytocin receptor gene affect baseline amygdala reactivity and the magnitude of social buffering of the stress response.
Lower OXTR expression or reduced receptor binding affinity predicts more pronounced amygdala reactivity to threat and reduced responsiveness to the calming effects of social contact.
These variants moderate both PTSD risk after trauma exposure and the magnitude of therapeutic response to coregulatory interventions. R
CRHR1 (CRH receptor 1) variants:
CRHR1 genetic variation is associated with altered cortisol response to psychosocial stress and moderates PTSD risk after trauma exposure.
Specific CRHR1 variants (rs12938031, rs4792887) increase PTSD risk through impaired cortisol feedback mechanisms.
These variants moderate the stress-physical health association across the lifespan. R
FKBP5 (rs1360780, rs4713916, rs3800373):
FKBP5 encodes FKBP51, a negative regulator of glucocorticoid receptor sensitivity.
The T allele of rs1360780 leads to greater FKBP5 induction following glucocorticoid receptor activation, impairing GR sensitivity.
T allele carriers with childhood trauma show significant FKBP5 demethylation, increasing FKBP51 expression, increasing GR resistance, and amplifying the HPA axis stress response in a pattern that persists epigenetically into adulthood. R
FKBP5 variants are among the most robustly associated genetic risk factors for PTSD, particularly in individuals with early life adversity. R
NR3C1 (glucocorticoid receptor gene):
Epigenetic modification of the NR3C1 promoter region by early life stress reduces GR expression in the hippocampus and PFC, impairing the cortisol feedback signal and contributing to HPA axis dysregulation that overlaps with both PTSD and the impaired coregulatory capacity associated with early developmental trauma. R
SLC6A4 (serotonin transporter, 5-HTTLPR):
The short (s) allele of 5-HTTLPR is associated with HPA axis hyperreactivity to social stress and increased amygdala reactivity to emotional stimuli.
This serotonin system genetic architecture directly influences the amygdala responsiveness that is central to PTSD and faulty neuroception, connecting the serotonin system's genetic variation to autonomic regulation and PTSD susceptibility. R
BDNF Val66Met (rs6265):
Brain-derived neurotrophic factor (BDNF) is essential for fear extinction learning and vmPFC-amygdala connectivity.
The Met allele of BDNF Val66Met is associated with reduced activity-dependent BDNF secretion, impaired fear extinction, reduced hippocampal volume, and more persistent PTSD following trauma exposure.
Given that EMDR and exposure therapy work through activating extinction learning circuits, BDNF Val66Met Met/Met carriers may show slower response to extinction-based therapies and may benefit from adjunctive approaches that support BDNF signaling (exercise, which robustly increases BDNF). R
More Research
- Measuring autonomic state as a treatment outcome. HRV is measurable, objective, and sensitive to autonomic recalibration.
The field is slowly moving toward including HRV as a primary or co-primary outcome measure in PTSD treatment trials rather than relying only on symptom questionnaires.
Tracking resting RMSSD and HF-HRV before and after intervention provides a biological marker that is independent of reporting bias and captures changes in autonomic flexibility that may precede symptom improvement. R
For biomarker testing, HRV monitoring with a consumer-grade chest strap or optical sensor provides accessible longitudinal data.
A WHOOP band or similar HRV monitor worn overnight captures resting HRV and provides a reliable trend metric.
- The sequence problem in trauma treatment. Standard first-line trauma therapies (prolonged exposure, CPT, EMDR) require some degree of window of tolerance to be effective.
People with severely dysregulated ANS cannot tolerate the activation that exposure-based approaches require.
The emerging model prioritizes autonomic stabilization first (HRV biofeedback, somatic experiencing, VNS) before trauma processing, creating the neurophysiological conditions that allow cognitive and narrative-level interventions to land. R
- Long COVID and PTSD-like autonomic dysregulation. Post-COVID autonomic dysfunction (reduced HRV, orthostatic intolerance, persistent sympathetic activation) overlaps extensively with the PTSD autonomic profile.
Both conditions involve reduced vagal tone, HPA axis dysregulation, and elevated neuroinflammation.
Whether HRV biofeedback, vagal stimulation, and somatic approaches proven in PTSD are transferable to long COVID autonomic dysregulation is an active research question with mechanistic justification. R
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Lion's Mane
1000mg/day
Omega-3 (DHA)
2g/day
Phosphatidylserine
100mg 3x/day