Tocopherols: Why Vitamin E Is Not One Thing And Why Alpha Alone Is A Problem
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Most vitamin E supplements contain only alpha-tocopherol, the form that dominates human plasma, and taking it in isolation may actively deplete the forms that do the anti-inflammatory and anti-cancer work.
In this post, we will discuss the four tocopherol forms, how they differ structurally and functionally, how the liver selectively retains alpha-tocopherol via a specific transfer protein, what gamma and delta tocopherols do that alpha cannot, why high-dose alpha-tocopherol supplementation displaces the other forms, and how to supplement this family correctly.
What Tocopherols Are: The Eight-Member Vitamin E Family
Vitamin E is not a single compound.
It is a collective term for eight structurally related fat-soluble molecules produced exclusively by photosynthetic organisms (plants, algae, and cyanobacteria). R
The family divides into two subfamilies: tocopherols (saturated phytyl side chain) and tocotrienols (unsaturated, three double-bond side chain). R
Within each subfamily there are four isomers: alpha (α), beta (β), gamma (γ), and delta (δ), named for the number and position of methyl groups on the chromanol ring. R
This post focuses on the tocopherols specifically.
The conventional nutritional framing treats vitamin E and alpha-tocopherol as interchangeable.
That framing is wrong, and it is driving supplement recommendations that may actively impair the biological functions that make the broader vitamin E family important. R
More than 95% of all vitamin E research has focused exclusively on alpha-tocopherol. R
The result is that the other forms remain poorly understood in clinical practice despite having distinct and in some cases superior biological activities.
Structure Of The Four Tocopherols
All four tocopherols share the same chromanol ring (the aromatic ring carrying the reactive hydroxyl group responsible for free radical scavenging) attached to a saturated 16-carbon phytyl side chain. R
The four isomers differ only in the number of methyl groups at positions 5, 7, and 8 of the chromanol ring: R
α-tocopherol: methyl groups at positions 5, 7, and 8 (fully methylated; highest alpha-TTP affinity, highest classical antioxidant potency)
β-tocopherol: methyl groups at positions 5 and 8 only (lowest biological activity among the four)
γ-tocopherol: methyl groups at positions 7 and 8 only (position 5 is unsubstituted; this free position enables unique reactions with reactive nitrogen species)
δ-tocopherol: methyl group at position 8 only (least methylated; lowest alpha-TTP affinity; strongest anti-proliferative and peroxisome proliferator-activated receptor-gamma (PPAR-γ) activating activity among the tocopherols)
The absence of a methyl group at position 5 in gamma and delta tocopherols is the structural reason they can chemically react with reactive nitrogen species (RNS) in ways that alpha-tocopherol cannot. R
Position 5 in alpha-tocopherol is blocked by a methyl group, preventing the nitrogen-trapping chemistry that makes gamma-tocopherol a functionally distinct molecule. R
How The Body Handles Tocopherols: Absorption And The alpha-TTP Bottleneck
All four tocopherols are absorbed non-selectively from the small intestine, packaged into chylomicrons, and delivered to the liver. R
Inside the liver, the discrimination begins.
Alpha-tocopherol transfer protein (α-TTP), encoded by the TTPA gene on chromosome 8q13.1-13.3, is a cytosolic liver protein that selectively binds RRR-α-tocopherol (the all-natural-(R,R,R) stereoisomer) from among all incoming tocopherol forms and packages it into nascent very low-density lipoprotein (VLDL) for secretion into the circulation. R R
α-TTP catalyzes the vectorial transport of alpha-tocopherol from the hepatic endocytic compartment to the plasma membrane by targeting phosphatidylinositol phosphates (PIPs) including PI(4,5)P2. R
The relative binding affinities of α-TTP for different tocopherols are: α > β > γ > δ. R
Gamma and delta tocopherols bind α-TTP poorly, are not efficiently incorporated into VLDL, and are instead excreted into bile or metabolized. R
The consequence: alpha-tocopherol is the dominant form in human plasma and tissues because of hepatic selection, not because it is metabolically superior to the other forms.
The consequence for supplements: when someone takes high-dose alpha-tocopherol, α-TTP preferentially packages it into VLDL, alpha-tocopherol saturates the transport system, and gamma and delta tocopherols are displaced from circulation and excreted more rapidly. R
Mutations in TTPA cause ataxia with vitamin E deficiency (AVED), an autosomal recessive neurological disorder characterized by progressive spinocerebellar ataxia, loss of position sense, and very low plasma alpha-tocopherol despite normal dietary intake. R
More than 20 distinct TTPA mutations have been identified in AVED patients worldwide. R
TTPA expression is induced by oxidative stress, hypoxia, PPARα and RXR agonists, and elevated cAMP levels, regulated at least in part through the cyclic AMP response element-binding protein (CREB) transcription factor, suggesting α-TTP levels respond to the body's antioxidant demand. R
What Alpha-Tocopherol Does
Alpha-tocopherol (αT) is the principal chain-breaking lipid antioxidant in plasma and cell membranes. R
It intercepts lipid peroxyl radicals (LOO•) in the lipid bilayer, donating a hydrogen atom from its phenolic hydroxyl group to break the radical chain and prevent propagation of lipid peroxidation. R
The relative antioxidant potency ratios of the four tocopherols in micellar dispersion are approximately 100:21:20:2.9 for α:β:γ:δ, which correlates with their differing degrees of methylation. R
Beyond antioxidant function, alpha-tocopherol acts through non-antioxidant signaling: R
Protein kinase C (PKC) inhibition: αT inhibits PKC activity in smooth muscle cells, platelets, and monocytes, which has downstream effects on cell proliferation, inflammatory signaling, and platelet aggregation. R
Prostacyclin regulation: αT increases expression of two enzymes that suppress arachidonic acid metabolism, increasing prostacyclin (PGI2) release from endothelium, producing vasodilation and inhibiting platelet aggregation. R
Tocopherol-associated protein (TAP): a hepatic protein with sequence similarity to α-TTP that binds alpha-tocopherol (but not other isoforms) and functions as a ligand-dependent transcriptional activator, suggesting alpha-tocopherol directly regulates gene expression through nuclear signaling. R
The recommended dietary allowance (RDA) for vitamin E is defined as 15 mg of alpha-tocopherol per day for adults, and alpha-tocopherol is the only form recognized to meet this requirement. R
More than 90% of American adults do not meet the estimated average requirement for vitamin E. R
What Gamma-Tocopherol Does Differently
Gamma-tocopherol is the most abundant form of vitamin E in the American diet (primarily from soybean, canola, and corn oils), yet plasma levels of gamma-tocopherol are far lower than alpha-tocopherol because α-TTP does not efficiently export it. R
Americans consume an estimated 2 to 4 times more gamma-tocopherol than alpha-tocopherol by dietary intake, yet plasma concentrations reflect the opposite, a consequence of the hepatic α-TTP filter. R
Gamma-tocopherol has at least three biological activities that alpha-tocopherol does not share:
1. Reactive Nitrogen Species Trapping
The unsubstituted position 5 on the gamma-tocopherol chromanol ring reacts with nitrogen dioxide (NO2), peroxynitrite (ONOO-), and other reactive nitrogen species to form 5-nitro-gamma-tocopherol (5-NO-γT). R R
Alpha-tocopherol cannot perform this reaction because position 5 is blocked by a methyl group. R
Peroxynitrite is a potent oxidant and nitrating agent formed when nitric oxide reacts with superoxide, and it is a key driver of inflammatory tissue damage. R
The trapping of reactive nitrogen species by gamma-tocopherol makes it functionally complementary to alpha-tocopherol, which traps reactive oxygen species (lipid peroxyl radicals) but is largely ineffective against nitrogen-based reactive species. R
Plasma 5-nitro-gamma-tocopherol is elevated in patients with coronary heart disease, providing in vivo evidence that this trapping reaction occurs under inflammatory conditions. R
2. Cyclooxygenase-2 (COX-2) Inhibition And The gamma-CEHC Metabolite
Gamma-tocopherol is metabolized by CYP4F2 (cytochrome P450 4F2) via omega-hydroxylation of the side chain, ultimately producing the water-soluble terminal metabolite gamma-CEHC (2,7,8-trimethyl-2-(beta-carboxyethyl)-6-hydroxychroman). R
A landmark PNAS study (Jiang, Ames et al., 2000) demonstrated that gamma-tocopherol reduced prostaglandin E2 (PGE2) synthesis in lipopolysaccharide (LPS)-stimulated macrophages with an IC50 of approximately 7.5 μM, and in IL-1β-treated human epithelial cells with an IC50 of approximately 4 μM. R
Alpha-tocopherol at 50 μM produced only about 25% inhibition of PGE2 in macrophages and no inhibition at all in epithelial cells. R
The inhibitory effects of gamma-tocopherol and gamma-CEHC on PGE2 production act directly on COX-2 enzyme activity, not on COX-2 protein expression or substrate availability. R
The metabolite gamma-CEHC also has an IC50 of approximately 30 μM for COX-2 inhibition. R
Longer-chain gamma-tocopherol metabolites, particularly 13′-carboxychromanol (13′-COOH), are even more potent inhibitors, blocking both COX-1/COX-2 and 5-lipoxygenase (5-LOX) simultaneously. R
Gamma-tocopherol also blocks 5-LOX translocation from cytosol to nucleus in leukocytes (by blocking ionophore-stimulated calcium influx and downstream JNK phosphorylation), suppressing leukotriene B4 (LTB4) formation. R
3. The LLU-alpha Natriuretic Factor
Gamma-CEHC was identified as LLU-alpha (Loma Linda University-alpha), a natriuretic factor isolated from human uremic urine after decades of search for the “natriuretic hormone” that regulates extracellular fluid volume. R
LLU-alpha/gamma-CEHC is natriuretic through inhibition of the 70 pS potassium channel in the thick ascending limb of the loop of Henle in the kidney, not through Na+/K+-ATPase inhibition as previously hypothesized for the natriuretic hormone. R
The S-enantiomer is the most potent known inhibitor of this channel, and the corresponding alpha-tocopherol metabolite has no equivalent activity. R
This makes gamma-tocopherol the only known vitamin whose catabolic metabolite functions as an endogenous hormone-like natriuretic factor with defined renal physiology, which makes adequate gamma-tocopherol intake potentially relevant to blood pressure and fluid volume regulation. R
What Delta-Tocopherol Does
Delta-tocopherol (δT) is the least studied and most recently appreciated form.
It is the least methylated tocopherol (methyl at position 8 only), has the lowest affinity for α-TTP, and therefore reaches the lowest plasma and tissue concentrations after ingestion compared with alpha or gamma. R
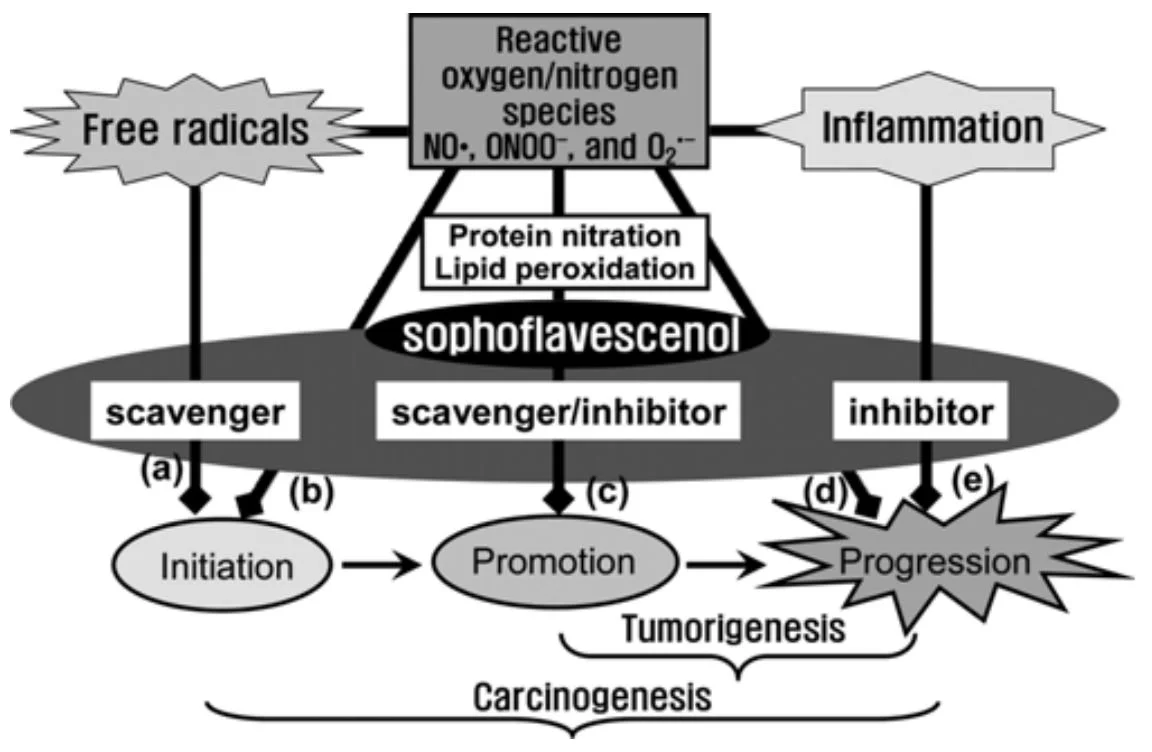
Despite low systemic levels, delta-tocopherol shows the strongest anti-proliferative and anti-carcinogenic activities among the tocopherols in both in vitro and animal models.
In an azoxymethane colon carcinogenesis model, delta-tocopherol treatment decreased aberrant crypt foci by 62%, a stronger inhibition than gamma-tocopherol and significantly stronger than alpha-tocopherol, which showed no inhibition. R
In lung cancer xenograft models, delta-tocopherol at 0.17% dietary supplementation was more active than alpha or gamma-tocopherol in inhibiting tumor growth. R
Delta-tocopherol mechanisms that distinguish it from alpha:
PPAR-γ activation: delta-tocopherol (and gamma-tocopherol) but not alpha-tocopherol activate peroxisome proliferator activated receptor-gamma (PPAR-γ), a nuclear receptor with anti-proliferative, pro-differentiating, and anti-estrogenic effects. R
Estrogen antagonism: in breast cancer cell models, delta and gamma-tocopherols but not alpha-tocopherol antagonize estrogen action and suppress ER-α protein expression and p-Akt signaling. R
Endothelial anti-angiogenic activity: delta-tocopherol at 40 μM decreased blood endothelial cell invasiveness and increased permeability in ways that gamma and alpha-tocopherol did not. R
TNF-α-induced VCAM-1 suppression: alpha, gamma, and delta tocopherols all dose-dependently reduce TNF-alpha-induced expression of VCAM-1 (vascular cell adhesion molecule 1) in blood endothelial cells, which is relevant to atherosclerosis initiation. R
The Problem With Alpha-Only Supplementation
This is the most clinically important section of this post.
Supplementation with high-dose alpha-tocopherol alone depletes gamma-tocopherol.
In a cross-sectional survey of 86 elderly persons, subjects with elevated plasma alpha-tocopherol had significantly depressed plasma gamma-tocopherol. R
When eight human volunteers were given 1200 International Units (IU) of all-rac-alpha-tocopherol daily for 8 weeks, plasma gamma-tocopherol fell to 30 to 50% of baseline values in all subjects while alpha-tocopherol increased 200 to 400% above initial values. R
Multiple subsequent studies and meta-analyses confirmed that alpha-tocopherol supplementation reduces serum concentrations of gamma and delta tocopherol in humans. R
The mechanism: alpha-tocopherol competes with gamma and delta tocopherol for α-TTP-mediated VLDL packaging, for lipoprotein binding sites in plasma, and probably for uptake into extrahepatic tissues. R
This explains the failure of large-scale alpha-tocopherol-only clinical trials.
The SELECT trial (Selenium and Vitamin E Cancer Prevention Trial) used 400 IU of alpha-tocopherol daily and found no reduction in prostate cancer; follow-up data suggested a slight increase in risk. R
One plausible interpretation: the high dose of alpha-tocopherol (400 IU/day) suppressed plasma and tissue gamma-tocopherol, eliminating the anti-inflammatory (COX-2 inhibition, nitrogen species trapping) and anti-proliferative activities that gamma-tocopherol provides. R
In contrast, lower-dose alpha-tocopherol (50 IU/day, the dose used in the Finnish ATBC study) was associated with decreased prostate cancer incidence, possibly because this dose did not suppress gamma-tocopherol to the same degree. R
The correct supplement approach: use mixed tocopherols enriched in gamma and delta tocopherols, not isolated alpha-tocopherol at high doses.
Supplementation with gamma-tocopherol increases both gamma and alpha plasma levels. R
Supplementation with alpha-tocopherol only increases alpha while depressing gamma and delta. R
On natural vs. synthetic alpha-tocopherol:
Natural alpha-tocopherol (RRR-α-tocopherol, labeled as d-α-tocopherol) has a single stereoisomeric configuration at the 2, 4′, and 8′ positions. R
Synthetic alpha-tocopherol (all-rac-α-tocopherol, labeled as dl-α-tocopherol) is an equal mixture of eight stereoisomers. R
Alpha-TTP has stereospecificity for the RRR configuration, which means a given weight of synthetic alpha-tocopherol provides approximately half the bioavailable activity of the same weight of natural RRR-α-tocopherol. R
When purchasing mixed tocopherols, look for products derived from soy or sunflower oil that specify ratios of gamma:delta:alpha, favoring higher gamma and delta fractions.
Natural Food Sources By Form
Alpha-tocopherol sources (highest first):
- Almonds (sunflower seeds provide the most per ounce of common nuts and seeds; 1 oz sunflower seeds provides roughly 2/3 of the adult RDA) R
- Hazelnuts (significant alpha-tocopherol; 1 oz provides greater than 20% RDA) R
- Olive oil (predominantly alpha-tocopherol among its tocopherol content) R
- Sunflower oil (over 93% of the tocopherols in sunflower oil are alpha-tocopherol) R
- Wheat germ oil (richest natural source of vitamin E; approximately 20 mg alpha-tocopherol per tablespoon, or 135% of daily value) R
Gamma-tocopherol sources (the major US dietary tocopherol by intake weight):
- Black walnuts (28 mg/100g gamma-tocopherol, highest of common nuts) R
- English walnuts and flaxseed (approximately 20 mg/100g gamma-tocopherol) R
- Pecans (approximately 24 mg/100g gamma-tocopherol) R
- Pistachios (approximately 22 mg/100g gamma-tocopherol) R
- Soybean oil (gamma-tocopherol content is approximately 7-fold higher than alpha-tocopherol in soybean oil) R
- Canola oil (gamma-tocopherol up to 2.7-fold higher than alpha-tocopherol) R
Delta-tocopherol sources:
Delta-tocopherol is present in significant concentrations in soybean, corn, and canola oils, and in lower quantities in sesame seeds and pumpkin seeds. R
Key insight on American diets: because soybean oil dominates US oil consumption (three-quarters of consumed oil), Americans are already consuming 2 to 4 times more gamma-tocopherol than alpha-tocopherol from diet, but the α-TTP hepatic filter prevents this dietary gamma-tocopherol from accumulating proportionally in plasma. R
Vitamin E is fat-soluble and absorbs poorly without dietary fat; always consume food sources with fat or take oil-based supplements with a fat-containing meal. R
How To Supplement: Protocol
1. Use Mixed Tocopherols Enriched In Gamma And Delta
The goal is to increase all four tocopherol forms simultaneously, not to drive alpha higher at the expense of gamma and delta.
Look for products that provide a ratio with significant gamma and delta fractions, typically labeled as “mixed tocopherols” or “gamma-tocopherol complex.”
A gamma-rich mixed tocopherol (gamma-TmT) formula used in clinical cancer prevention models contained approximately 57% gamma, 24% delta, 13% alpha, and 1.5% beta. R
Mixed Tocopherols Gamma-E Complex
2. If Using Alpha-Tocopherol, Use RRR (Natural) Form At Low Dose
If using an alpha-tocopherol supplement specifically, choose the natural RRR-α-tocopherol (d-alpha-tocopherol) form over synthetic all-rac-alpha-tocopherol (dl-alpha-tocopherol), which has approximately twice the bioavailable activity per milligram. R
Keep alpha-tocopherol supplementation to modest doses (100 to 200 IU range) if using it in isolation, as doses above 400 IU/day appear to suppress gamma-tocopherol reliably. R
Natural Vitamin E d-Alpha Tocopherol 200 IU
3. Prioritize Dietary Sources With The Full Tocopherol Spectrum
Whole-food sources deliver mixed tocopherols in natural ratios without the suppression effect of pharmacological alpha-tocopherol supplementation.
Walnuts, pecans, and sunflower seeds together cover both alpha and gamma-rich fractions.
A tablespoon of wheat germ oil covers the alpha side without driving the extreme plasma alpha levels that suppress gamma.
4. Take With Fat
Vitamin E absorption requires dietary fat for chylomicron packaging. R
Always take tocopherol supplements with a meal containing meaningful fat content (olive oil, avocado, nuts, or fatty fish).
What To Stay Away From
High-dose isolated alpha-tocopherol supplements (400 IU/day or more): reliably suppress plasma and tissue gamma and delta tocopherol, eliminating the anti-inflammatory COX-2 inhibition, nitrogen species trapping, and anti-proliferative PPAR-γ activity that these forms provide. R R
Synthetic dl-alpha-tocopherol (all-rac): only half the biological potency of the natural RRR form per milligram; provides four non-natural stereoisomers that are not recognized by α-TTP. R
Vitamin E supplements without fat: tocopherols are fat-soluble and require co-ingestion of fat for absorption via chylomicron formation. R
Very high-dose alpha-tocopherol if on blood thinners: high-dose supplemental alpha-tocopherol may interfere with vitamin K absorption and increase bleeding risk; the tolerable upper intake level is 1,000 mg per day of alpha-tocopherol. R (Discuss with your prescriber before supplementing if you take anticoagulants.)
Testing
Blood Markers
Standard vitamin E testing reports total serum alpha-tocopherol, which reflects α-TTP export activity rather than whole-body tocopherol status across all forms.
Because gamma and delta tocopherols are not efficiently retained by α-TTP, they can be genuinely low even when serum alpha-tocopherol is normal or elevated.
The alpha-to-gamma tocopherol ratio in plasma is a more informative marker than either form alone; elevated ratios (indicating low gamma relative to alpha) have been associated with colorectal adenoma incidence and inflammatory states. R
Elevated plasma gamma-tocopherol with low alpha is associated with inflammatory markers and may indicate inadequate alpha-tocopherol intake alongside ongoing inflammatory consumption of gamma-tocopherol. R
Functional Lab Panels
I use the Nutrient Zoomer (Vibrant Wellness) to assess alpha and gamma tocopherol levels alongside other fat-soluble vitamins, minerals, and oxidative stress markers in the same panel.
The Cellular Zoomer (Vibrant Wellness) provides organic acid and oxidative stress markers that can reflect whether antioxidant systems are under load, which contextualizes tocopherol status.
For comprehensive cardiovascular and inflammatory context (relevant to interpreting tocopherol needs in vascular disease), I use the Cardio Zoomer.
Mechanisms Of Action
Simple:
- All four tocopherols embed in cell membranes and lipoproteins and donate hydrogen atoms to stop lipid peroxidation chain reactions; alpha-tocopherol is the most potent at this and is the dominant form in plasma.
- Gamma and delta tocopherols have a free position on their ring that allows them to chemically trap reactive nitrogen species (like peroxynitrite) that alpha-tocopherol cannot react with.
- Gamma-tocopherol and its metabolite gamma-CEHC directly inhibit COX-2 enzyme activity, reducing prostaglandin E2 production in a way that alpha-tocopherol does not.
- The liver selectively exports alpha-tocopherol into VLDL via a specific transfer protein (alpha-TTP), which is why alpha dominates plasma regardless of dietary ratios.
- Taking large doses of alpha-tocopherol saturates alpha-TTP, displacing gamma and delta from circulation and eliminating their functions.
Advanced:
- Alpha-TTP mechanism: Alpha-TTP is a member of the CRAL-TRIO lipid-binding protein family. R It binds RRR-α-tocopherol in the endocytic compartment of hepatocytes, catalyzes vectorial transport to the plasma membrane by directly interacting with phospholipid bilayers and targeting PI(4,5)P2 at the plasma membrane. R The protein then facilitates transfer into nascent VLDL before secretion. R Alpha-TTP expression is induced by oxidative stress through CREB-mediated transcription in hepatocytes, creating a feedback mechanism that increases alpha-tocopherol export during high oxidative demand. R
- Lipid peroxidation chain-breaking: Tocopherols donate a hydrogen atom from the chromanol hydroxyl group to lipid peroxyl radicals (LOO•), forming a tocopheroxyl radical that is then reduced back to tocopherol by ascorbic acid (vitamin C) or glutathione. R The reaction rate constant for alpha-tocopherol with peroxyl radicals in membranes is approximately 100-fold higher than for gamma or delta. R
- Gamma-tocopherol nitrogen trapping: The free C-5 position on gamma-tocopherol chromanol ring reacts with NO2 radical and peroxynitrite to form 5-nitro-gamma-tocopherol, a stable product. R This reaction irreversibly consumes gamma-tocopherol but simultaneously detoxifies the reactive nitrogen species. R Elevated 5-nitro-gamma-tocopherol in plasma is measurable by LC-MS and functions as a biomarker of in vivo nitrogen radical burden and gamma-tocopherol consumption. R
- Gamma-CEHC COX-2 inhibition: CYP4F2 initiates side-chain omega-hydroxylation of gamma-tocopherol at the terminal methyl, producing 13′-hydroxychromanol, which undergoes sequential beta-oxidation steps to form intermediate carboxychromanols and ultimately gamma-CEHC. R The intermediate 13′-carboxychromanol (13′-COOH) is a more potent dual COX-1/COX-2 and 5-LOX inhibitor than gamma-CEHC. R The COX-2 inhibition is at the enzyme activity level (not expression), acting at or near the active site of the cyclooxygenase. R
- LLU-alpha natriuretic mechanism: Gamma-CEHC (LLU-alpha) inhibits the 70 pS K+ channel in the apical membrane of the thick ascending limb of the loop of Henle, reducing potassium recycling and therefore reducing the driving force for NaCl reabsorption, producing natriuresis. R The S-enantiomer (the stereoisomer produced from natural S-gamma-tocopherol) is the active form; the analogous alpha-tocopherol metabolite alpha-CEHC shows no equivalent channel inhibitory activity. R
- Alpha-tocopherol PKC inhibition: Alpha-tocopherol directly inhibits protein kinase C (PKC) activity, particularly in smooth muscle cells and platelets. R PKC inhibition reduces cell proliferation signaling, platelet activation, and monocyte-endothelial adhesion. This occurs through non-antioxidant mechanisms including inhibition of PKC-alpha via diacylglycerol displacement. R
- Delta and gamma PPAR-γ activation: Delta and gamma tocopherols activate PPAR-γ (peroxisome proliferator-activated receptor gamma) through direct ligand binding of this nuclear receptor. R PPAR-γ activation induces differentiation and apoptosis in cancer cells, antagonizes estrogen receptor signaling, and activates p21 and p27 cell cycle arrest proteins. R Alpha-tocopherol does not activate PPAR-γ at physiological concentrations. R
- Alpha-tocopherol depletion of gamma-tocopherol: The molecular mechanism is competition at multiple steps: (1) both forms compete for the same α-TTP binding site in hepatocytes, with alpha having superior affinity; (2) high circulating alpha-tocopherol competes with gamma-tocopherol for lipoprotein binding sites in plasma; (3) in extrahepatic tissues, elevated cellular alpha-tocopherol may accelerate gamma-tocopherol catabolism by upregulating CYP4F2-mediated omega-hydroxylation. R R
Genetics
TTPA (Alpha-Tocopherol Transfer Protein)
TTPA encodes alpha-TTP, located on chromosome 8q13.1-13.3. R
Loss-of-function mutations cause ataxia with vitamin E deficiency (AVED, OMIM 277460), an autosomal recessive neurological disorder characterized by progressive spinocerebellar ataxia, loss of position sense, loss of vibration sense, and very low plasma alpha-tocopherol. R
AVED is caused by failure of hepatic alpha-tocopherol incorporation into VLDL; absorption is normal but systemic distribution fails. R
More than 20 distinct TTPA mutations have been identified. R
R59W, E141K, R221W: associated with early-onset severe AVED (typically presenting in the first decade). R
H101Q, A120T, R192H: associated with later-onset, milder AVED; mutations that impair membrane interaction and tocopherol transfer to a lesser degree. R
A linear correlation exists between plasma alpha-tocopherol levels and TTPA gene dosage (TTP+/+, TTP+/-, TTP-/- mice show proportional differences), confirming that α-TTP is the primary determinant of systemic alpha-tocopherol status in mammals. R
Common non-pathogenic TTPA SNPs contribute to normal individual variation in plasma alpha-tocopherol levels.
CYP4F2 (Gamma-Tocopherol Catabolism)
CYP4F2 encodes the enzyme that initiates side-chain catabolism of gamma, delta, and alpha tocopherols via omega-hydroxylation. R
CYP4F2 variants affect the rate of gamma-tocopherol catabolism and therefore influence plasma gamma-tocopherol levels and the production of the anti-inflammatory metabolites gamma-CEHC and 13′-COOH. R
CYP4F2 rs2108622: a known functional variant associated with reduced CYP4F2 enzyme activity; individuals carrying this variant may catabolize gamma-tocopherol more slowly, potentially accumulating higher gamma-tocopherol levels and metabolites. R
This variant is also relevant to vitamin K metabolism (CYP4F2 catabolizes vitamin K1), linking tocopherol and vitamin K pathways at the genomic level. R
More Research
- Alpha-tocopherol at the α/γ-tocopherol plasma ratio level is a more sensitive marker of colorectal adenoma risk than absolute concentrations of either form alone; the ratio reflects the suppressive effect of dietary and supplemental alpha on gamma, and may index the individual's loss of COX-2 inhibitory and nitrogen-trapping capacity. R
- Beta-tocopherol is consistently the least abundant tocopherol in human plasma and tissues and has the lowest biological activity among the four; it is poorly absorbed and does not accumulate to physiologically meaningful levels even with dietary intake. R
- Delta-tocopherol is more active than alpha or gamma tocopherol in inhibiting lung tumorigenesis in xenograft mouse models, yet despite this, it is never mentioned in clinical supplement recommendations and reaches the lowest plasma levels of the four forms because of α-TTP's very low affinity for it. R
- Elevated plasma gamma-tocopherol with low alpha-tocopherol is associated with inflammatory markers including CRP and IL-6, and with decreased 25-OH vitamin D; gamma elevation in this context reflects inflammatory consumption of gamma-tocopherol's nitrogen-trapping capacity rather than gamma sufficiency. R
- TTPA expression is induced by oxidative stress and hypoxia through CREB-mediated transcriptional activation, representing a feedback loop in which cellular oxidative burden triggers increased alpha-tocopherol export from the liver to increase antioxidant delivery to peripheral tissues. R
- Gamma-tocopherol supplementation in humans simultaneously increases both gamma and alpha-tocopherol plasma levels, the opposite relationship to alpha-tocopherol supplementation, which suppresses gamma. R This suggests that gamma-rich mixed tocopherol supplements are superior to alpha-only products for maintaining the complete functional tocopherol spectrum.
For biomarker testing I use the Nutrient Zoomer (Vibrant Wellness) to assess alpha and gamma tocopherol levels alongside the full fat-soluble vitamin and oxidative stress panel.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Electrolyte Complex
1 scoop/day
CoQ10
200mg/day
Magnesium Glycinate
400mg at bedtime