The Sleep Supplements Guide: Melatonin, Magnesium Glycinate, And Beyond
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Poor sleep is one of the most common complaints I hear from people dealing with chronic illness, post-viral syndromes, dysautonomia, and the general wear and tear of modern life.
In this post, we will discuss the evidence behind the most popular and research-backed sleep supplements, how they work, who they help most, how to combine them safely, and when to look deeper at root causes.

What Is Sleep (Brief Overview)
Sleep is not a passive off-state.
It is an active, architecturally complex physiological process organized into roughly 90-minute cycles of Non-Rapid Eye Movement (NREM) and Rapid Eye Movement (REM) sleep. R
NREM sleep, particularly slow-wave (deep) sleep, is when the glymphatic system clears metabolic waste from the brain, growth hormone is released, and cellular repair processes ramp up. R
REM sleep is when memory consolidation, emotional processing, and synaptic pruning occur. R
The two main challenges people face are sleep-onset insomnia (difficulty falling asleep) and sleep-maintenance insomnia (difficulty staying asleep or waking too early), and different supplements target each type differently.
I have written extensively about my personal sleep protocol in how I get 3-4 hours of deep sleep every night, and about the circadian machinery that drives it all in zeitgebers and circadian rhythm.
Natural Approaches Before Supplements
Supplements should never be the first lever you pull.
Sleep is a systems-level phenomenon that depends on light exposure, temperature, movement, and gut health.
Before reaching for a bottle, address these foundational factors.
Morning light exposure: Bright light within 30-60 minutes of waking sets the circadian clock for the entire day. R
Consistent sleep schedule: Bedtime and wake time within the same 30-minute window, seven days a week, is the single most effective behavioral intervention for insomnia. R
Temperature regulation: Core body temperature must drop 0.5-1.0 degrees Celsius for sleep onset to occur, which is why cooling the bedroom (65-68 degrees Fahrenheit) and taking a warm bath 90 minutes before bed (which triggers a compensatory cooling rebound) are evidence-based. R
Gut microbiome: The gut-brain axis directly regulates sleep via serotonin, GABA, and short-chain fatty acid signaling, and dysbiosis is a well-documented driver of poor sleep quality. R
I covered this connection in detail in gut microbiome and insomnia.
Blood sugar stability: Nocturnal blood glucose dips trigger cortisol and adrenaline release that wake you up, which is why a low-carb or balanced-protein evening meal often improves sleep-maintenance insomnia. R
Red and near-infrared light: Exposure to red or near-infrared light before bed can increase ATP production in retinal mitochondria and support melatonin synthesis. R
I discussed the dosing parameters in red light therapy dose ceiling.
Limit blue light after sunset: Blue wavelengths suppress melatonin production at the retinal ganglion cell level via melanopsin, and blue-blocking glasses or device filters measurably improve sleep onset latency. R
Glymphatic support: The glymphatic system clears brain waste primarily during deep sleep, and hydration, head-of-bed elevation, and cervical mobility all affect its efficiency. R
I wrote about this in improve glymphatic system and AQP4 biohacks.
The Sleep Supplement Stack
The following supplements are listed alphabetically.
Each entry covers what the supplement does, the evidence, the dose range, and whether it primarily targets sleep onset or sleep maintenance.

Apigenin
Apigenin is a flavonoid found abundantly in chamomile, parsley, and celery that acts as a positive allosteric modulator of GABA-A receptors, producing mild anxiolytic and sedative effects without the dependency profile of benzodiazepines. R
Dietary apigenin intake positively correlates with sleep quality in a large cohort of adults, and chamomile extract (standardized to apigenin content) has been shown in clinical trials to improve sleep quality and reduce anxiety. R
Apigenin also inhibits the NAD-consuming enzyme CD38, which may have anti-aging effects independent of its sleep benefits. R
Target: Sleep onset (mild sedative, anxiolytic)
Dose: 50-100 mg of standardized apigenin extract, or 270-400 mg of chamomile extract (standardized to 1.0-1.2% apigenin), taken 30-60 minutes before bed
I covered this compound in depth in apigenin benefits and mechanisms.
Ashwagandha (For Cortisol)
Ashwagandha (Withania somnifera) is an adaptogenic herb whose primary sleep-relevant mechanism is modulation of the Hypothalamic-Pituitary-Adrenal (HPA) axis and reduction of serum cortisol. R
A 2022 meta-analysis of 12 randomized controlled trials (n = 1,002) found that ashwagandha supplementation significantly reduced serum cortisol by a weighted mean of 11-27.9% depending on dose and duration. R
A 2021 meta-analysis of 5 RCTs found statistically significant improvements in overall sleep quality, sleep onset latency, and total sleep time with ashwagandha versus placebo, with more pronounced effects at 600 mg daily and in participants with diagnosed insomnia. R
Ashwagandha is best suited for people whose sleep problems are driven by high stress and elevated evening cortisol rather than by circadian misalignment or blood sugar issues.
Target: Sleep onset (via cortisol reduction)
Dose: 300-600 mg of standardized KSM-66 or Sensoril extract, taken with the evening meal (not immediately before bed, as the cortisol-lowering effect takes weeks to build)
I have a full breakdown in ashwagandha benefits, mechanisms, and adaptogen profile.
CBD / CBN
Cannabidiol (CBD) and Cannabinol (CBN) are phytocannabinoids that interact with the Endocannabinoid System (ECS), which is distributed throughout the central nervous system and plays a role in regulating the sleep-wake cycle via CB1 receptors in the hypothalamus. R
CBD has more robust evidence for anxiety reduction than for direct sleep promotion, and at doses above 300 mg it may increase total sleep time in some populations, though the data are mixed. R
CBN has recently been studied in placebo-controlled trials.
A 2023 randomized trial (n = 293) found that 20 mg of CBN significantly reduced nighttime awakenings and overall sleep disturbance compared to placebo, though it did not improve sleep onset latency or wake-after-sleep-onset. R
A 2026 crossover trial using 300 mg CBN found significant increases in NREM stage 2 sleep, improved subjective sleep quality, and shorter time to fall asleep, though it did not reduce WASO at either 30 mg or 300 mg. R
CBN appears more useful for sleep maintenance than sleep onset, whereas CBD is more useful for the anxiety that prevents sleep onset.
Target: Sleep maintenance (CBN), sleep onset via anxiety reduction (CBD)
Dose: 20-100 mg CBN for maintenance; 25-300 mg CBD for anxiety.
Start low.
Quality and purity vary widely; third-party tested products only.
GABA
Gamma-Aminobutyric Acid (GABA) is the primary inhibitory neurotransmitter in the central nervous system.
Oral GABA supplementation is controversial because its ability to cross the Blood-Brain Barrier (BBB) in meaningful quantities is debated. R
Despite this, clinical studies using typical dietary doses (100-300 mg/day) have reported significant improvements in sleep outcomes, suggesting that its efficacy may rely on indirect mechanisms involving the gut-brain axis, enteric nervous system signaling, and vagal activation rather than direct CNS entry. R
GABA is generally safe and well-tolerated, but the evidence is weaker than for magnesium glycinate, L-theanine, or glycine.
Target: Sleep onset (mild relaxant)
Dose: 100-300 mg, taken 30-60 minutes before bed
Glycine
Glycine is the smallest amino acid and functions as both an inhibitory neurotransmitter in the spinal cord and brainstem and as a co-agonist at NMDA receptors in the suprachiasmatic nucleus (SCN). R
Glycine ingestion before bedtime significantly improves subjective sleep quality, reduces sleep onset latency, and decreases daytime sleepiness in human volunteers, as confirmed by polysomnography. R
The mechanism is primarily thermoregulatory: glycine activates NMDA receptors in the SCN, which triggers peripheral vasodilation and a drop in core body temperature, which is a prerequisite for sleep onset. R
A 2015 study established that these effects are mediated by NMDA receptors in the SCN shell and are abolished by SCN ablation. R
Target: Sleep onset
Dose: 3 grams taken 30-60 minutes before bed as a powder.
This is the dose used in all positive clinical trials.
Magnesium glycinate contains only about 200-500 mg of glycine per serving, so it is insufficient for the thermoregulatory mechanism.
L-Theanine
L-Theanine is a non-protein amino acid found almost exclusively in tea leaves (Camellia sinensis) that promotes a state of calm alertness by increasing alpha-wave activity in the brain. R
A 2021 triple-blind, placebo-controlled crossover study found that 200 mg of L-theanine significantly increased frontal region alpha power and reduced salivary cortisol compared to placebo in response to an acute stress challenge. R
A 2025 systematic review of L-theanine and sleep found that it reduces sleep onset latency and improves sleep quality, though the authors noted that many studies are small and effects are modest. R
A 2011 RCT in boys with ADHD found that 400 mg of L-theanine daily improved objective sleep quality (higher sleep efficiency, less wake after sleep onset). R
Unlike sedatives, L-theanine promotes relaxation without causing drowsiness, making it useful for people whose racing thoughts prevent sleep onset but who do not want next-day grogginess.
Target: Sleep onset (via relaxation and alpha-wave enhancement)
Dose: 100-400 mg, taken 30-60 minutes before bed.
Can also be taken during the day for calm focus.
I covered this in L-theanine benefits and mechanisms.
Magnesium Glycinate
Magnesium Glycinate (also called magnesium bisglycinate) is magnesium chelated to two glycine molecules, offering both the mineral's calming effects on the nervous system and a modest amount of glycine.
A 2025 randomized, double-blind, placebo-controlled trial (n = 155) found that 250 mg of elemental magnesium as magnesium bisglycinate significantly reduced Insomnia Severity Index scores compared to placebo at four weeks, with the most pronounced benefit in participants with low baseline dietary magnesium intake. R
Magnesium supports sleep through multiple pathways: it is a cofactor for GABA-A receptor function, it regulates NMDA receptor activity, it supports melatonin synthesis, and it modulates the HPA axis to reduce cortisol. R
Glycinate is the preferred form for sleep because it is well-absorbed, does not cause the laxative effect of citrate or oxide, and the glycine moiety provides additional sleep-supportive effects.
Older RCTs using 500 mg of elemental magnesium (as magnesium oxide) in elderly insomniacs also found significant increases in sleep time, sleep efficiency, and serum melatonin, plus reductions in serum cortisol. R
Target: Sleep onset and sleep maintenance (both)
Dose: 200-400 mg of elemental magnesium as glycinate, taken 30-60 minutes before bed
Magnesium L-Threonate
Magnesium L-Threonate is a patented form of magnesium (Magtein) that was developed at MIT with demonstrated ability to raise brain magnesium levels more effectively than other forms. R
A 2024 randomized controlled trial (n = 80) found that 1 g of magnesium L-threonate daily for 21 days significantly improved objective deep sleep score, REM sleep score, and subjective measures of upon-waking behavior, energy, and daytime productivity compared to placebo. R
A 2025-2026 RCT (n = 100) found that 2 g daily for 6 weeks improved overall cognition, working memory, and reaction time, plus subjective sleep-related impairment, though objective sleep measures from wearable trackers did not show group differences. R
Magnesium L-threonate may be the best option for those who want both cognitive enhancement and sleep support from their magnesium supplementation.
Target: Sleep onset and sleep quality, with additional cognitive benefits
Dose: 1-2 g daily (providing approximately 144-200 mg elemental magnesium), taken in divided doses or 30-60 minutes before bed
Melatonin
Melatonin is the master hormone of circadian timing, produced by the pineal gland in response to darkness and suppressed by light.
A meta-analysis of 19 studies involving 1,683 subjects found that exogenous melatonin modestly but significantly reduced sleep onset latency (by approximately 7 minutes), increased total sleep time (by approximately 8 minutes), and improved overall sleep quality. R
A dose-response meta-analysis of 26 RCTs found that the sleep-promoting effects of melatonin peak at 4 mg and that advancing the timing of administration to 3 hours before desired bedtime may be more effective than taking it 30 minutes before bed. R
Low-dose melatonin (0.3-0.5 mg) produces blood levels similar to endogenous nocturnal peaks and is less likely to cause next-day grogginess or circadian phase shifts than the common 3-10 mg doses found in most retail products. R
Target: Sleep onset (circadian phase-shifting)
Dose: 0.3-0.5 mg for circadian alignment, or 1-4 mg for sleep onset, taken 1-3 hours before desired bedtime.
Extended-release formulations may help with sleep maintenance.
I covered this in detail in benefits of melatonin.
Oleamide
Oleamide (9-octadecenamide) is a fatty acid amide that accumulates naturally in the cerebrospinal fluid during sleep deprivation and acts as an endogenous sleep-inducing molecule. R
Peripheral administration of oleamide to rats dose-dependently reduces motor activity and decreases sleep latency to 44-64% of control values without altering other sleep parameters. R
Oleamide is thought to act through the endocannabinoid system, enhancing serotonergic (5-HT) and GABAergic neurotransmission, and it also activates PPAR-alpha receptors, which may support hippocampal neurogenesis. R
Human clinical data on oral oleamide supplementation are extremely limited, and most of what we know comes from animal models.
Target: Sleep onset
Dose: There is no established human dose from clinical trials.
Most products recommend 50-300 mg, but the evidence base is thin.
Approach with caution.
Phosphatidylserine
Phosphatidylserine (PS) is a phospholipid concentrated in neuronal cell membranes that supports neurotransmitter signaling and cell communication.
Its primary sleep-relevant effect is blunting of the cortisol response to stress.
A 2008 double-blind, placebo-controlled crossover study found that 600 mg of phosphatidylserine per day for 10 days reduced peak exercise cortisol by approximately 39% and cortisol area-under-the-curve by approximately 35% in trained males. R
Phosphatidylserine is best suited for people whose sleep maintenance problems are driven by elevated evening or nighttime cortisol, particularly those in chronic stress states, overtraining, or perimenopause.
Target: Sleep maintenance (via cortisol reduction)
Dose: 300-600 mg daily, taken in the evening.
Effects build over 7-14 days and are not acute.
Taurine
Taurine is a conditionally essential amino acid that acts as a weak agonist at GABA-A receptors and an agonist at glycine receptors, producing inhibitory effects in the central nervous system. R
Taurine also modulates calcium signaling in neurons and has demonstrated sleep-promoting effects in animal models, increasing NREM sleep time and altering REM sleep latency. R
Human clinical data specific to sleep are limited, though taurine has a strong safety profile and is widely used in functional beverages and traditional medicine for its calming effects.
Taurine may be more useful as an adjunct in a stack than as a standalone sleep aid.
Target: Sleep onset (mild GABAergic)
Dose: 500-1,500 mg, taken 30-60 minutes before bed
I covered this in taurine benefits and mechanisms.
Tryptophan / 5-HTP
L-Tryptophan is an essential amino acid and the dietary precursor to serotonin, which is itself the precursor to melatonin.
5-Hydroxytryptophan (5-HTP) is the direct intermediate between tryptophan and serotonin, and it crosses the blood-brain barrier more efficiently than tryptophan itself.
A 2024 randomized controlled trial (n = 30 older adults) found that 100 mg of 5-HTP daily for 12 weeks significantly improved objective sleep latency and subjective sleep quality in poor sleepers, with greater benefits in those with lower baseline sleep quality. R
A separate 2019 crossover trial found that tryptophan (1,000 mg/day) improved objective sleep efficiency and wake after sleep onset across all participants, with a marginally significant improvement in subjective sleep quality in 5-HTTLPR S-allele carriers (a genetic variant associated with reduced serotonin transporter function). R
Serotonin syndrome risk: 5-HTP should NOT be combined with SSRI or SNRI antidepressants, St. John's Wort, MAO inhibitors, or other serotonergic drugs, as this can cause potentially life-threatening serotonin syndrome.
Target: Sleep onset (via serotonin and melatonin precursor loading)
Dose: Tryptophan 500-2,000 mg, or 5-HTP 50-100 mg, taken 30-60 minutes before bed on an empty stomach.
Start with the lowest dose.
Do not combine with serotonergic medications.
Valerian Root
Valerian Root (Valeriana officinalis) has been used as a sedative since the 18th century and acts by inhibiting sympathetic nervous system neurons through modulation of GABA. R
The evidence is mixed.
A 2006 meta-analysis of 16 RCTs (n = 1,093) found that valerian improved subjective sleep quality (relative risk of improved sleep = 1.8) but noted significant methodological problems and possible publication bias. R
A 2023 randomized, double-blind, placebo-controlled trial using a standardized valerian extract (n = 80) found significant improvements in PSQI scores, sleep latency measured by actigraphy, and subjective anxiety at 8 weeks. R
Valerian may require 2-4 weeks of consistent use before benefits become noticeable, which suggests its mechanism is not acute sedation but gradual modulation of GABAergic tone.
Withdrawal risk: Unlike benzodiazepines, valerian is not associated with classical dependence, but abrupt discontinuation after long-term high-dose use has been reported to cause rebound insomnia in some cases.
Target: Sleep onset (subjective quality)
Dose: 300-600 mg of standardized root extract (0.8% valerenic acid), taken 30-60 minutes before bed for 2-4 weeks minimum
Zinc
Zinc is an essential trace mineral that functions as a neuromodulator in the brain and is involved in the regulation of sleep through modulation of NMDA and GABA receptors. R
A systematic review of randomized controlled trials found that zinc supplementation (typically 30 mg/day) improved sleep quality, particularly sleep latency and subjective sleep quality, across multiple populations. R
A 2022 RCT in hemodialysis patients found that 30 mg of zinc gluconate for 12 weeks significantly improved PSQI scores. R
A 2025 meta-analysis of dietary supplement interventions found that zinc, tryptophan, vitamin D, and omega-3 were among the nutrients with the strongest evidence for sleep improvement. R
Zinc is best thought of as a foundational nutrient for sleep rather than a standalone sleep aid.
If you are zinc-deficient (which is common in chronic illness), supplementation may be transformative for sleep.
Target: Sleep onset and sleep maintenance (via neurotransmitter modulation)
Dose: 15-30 mg elemental zinc daily with food.
Long-term high-dose zinc can cause copper deficiency, so cycle or use a balanced mineral formula.
Ziziphus Jujuba (Suan Zao Ren)
Ziziphus Jujuba (sour jujube seed, Suan Zao Ren) is a traditional Chinese medicinal herb used for insomnia for millennia, with modern research identifying over 354 bioactive compounds including flavonoids and triterpenoids that upregulate GABA-A receptor expression. R
A randomized, double-blind, placebo-controlled crossover trial (n = 12) found that 2 g daily of Ziziphus spinosa seed for 4 weeks significantly improved PSQI scores compared to placebo, with improvements in total sleep time, sleep efficiency, and sleep onset latency. R
A 2026 clinical trial (n = 25) found that Ziziphus jujuba seed extract reduced sleep latency from 53 to 30 minutes and significantly improved subjective sleep quality. R
Ziziphus jujuba also upregulates Brain-Derived Neurotrophic Factor (BDNF), Glial Cell Line-Derived Neurotrophic Factor (GDNF), and Neurotrophin-3 (NT-3), making it a rare sleep aid with neurotrophic properties. R
Target: Sleep onset (via GABAergic and neurotrophic mechanisms)
Dose: 1-3 g of seed powder or extract, taken 30-60 minutes before bed
I covered this in depth in ziziphus jujuba, NGF, BDNF, GDNF, NT-3, NRF2, and sleep.

Combination Protocols
Stacking supplements that target different mechanisms often produces better results than any single agent.
Here are evidence-informed combinations for specific sleep presentations.
For Sleep Onset Insomnia (Racing Mind, Can't Fall Asleep)
L-Theanine 200 mg + Magnesium Glycinate 200 mg + Glycine 3 g
The L-theanine increases alpha waves and reduces cortisol, magnesium glycinate supports GABAergic tone and provides a small glycine contribution, and the full 3 g of glycine triggers the thermoregulatory cooling needed for sleep onset.
For Sleep Maintenance Insomnia (Waking At 2-3 AM, Can't Get Back To Sleep)
Phosphatidylserine 300 mg + Ashwagandha 300 mg + Magnesium L-Threonate 1 g
The phosphatidylserine and ashwagandha work synergistically to lower elevated cortisol (which typically drives early morning waking), while magnesium L-threonate supports brain magnesium levels for overnight neural stability.
For High-Cortisol / Stress-Driven Insomnia
Ashwagandha 600 mg KSM-66 (with evening meal) + Phosphatidylserine 400 mg (1 hour before bed)
The combination has been used in clinical contexts for HPA axis dysregulation, with the ashwagandha taking 4-8 weeks to show full effect and the phosphatidylserine working more quickly.
For Mild / Occasional Insomnia
Melatonin 300 mcg (0.3 mg) + L-Theanine 100 mg
This is a low-risk, low-dose combination for travel or occasional poor sleep that will not disrupt endogenous melatonin production or cause next-day grogginess.
For Gut-Related Sleep Disturbance
Zinc 15 mg + Magnesium Glycinate 200 mg + Ziziphus Jujuba 1 g
Zinc supports the gut barrier and acts as a neuromodulator, magnesium glycinate addresses the high prevalence of magnesium deficiency in GI conditions, and ziziphus jujuba provides GABAergic support with additional neurotrophic benefits.
Safety And Interactions
Not all sleep supplements are safe for everyone.
Here are the important cautions organized alphabetically.
5-HTP and SSRIs/SNRIs: 5-HTP combined with serotonergic antidepressants, St. John's Wort, or MAO inhibitors can cause serotonin syndrome, which is a medical emergency characterized by agitation, hyperthermia, tachycardia, and clonus.
Ashwagandha and thyroid medication: Ashwagandha can increase T4 conversion, so people on thyroid medication should monitor thyroid function and adjust dosage with their practitioner.
Ashwagandha and pregnancy: Ashwagandha is not recommended during pregnancy as it may stimulate uterine contractions.
CBN/CBD and liver enzymes: High-dose CBD can inhibit CYP450 liver enzymes, potentially altering metabolism of prescription medications including blood thinners, anti-epileptics, and some antidepressants.
Glycine and clozapine: Glycine can affect the efficacy of clozapine in people with schizophrenia.
Magnesium and antibiotics: Magnesium can chelate tetracycline and fluoroquinolone antibiotics, reducing absorption.
Magnesium and kidney disease: People with chronic kidney disease (CKD) should not take magnesium supplements without medical supervision, as impaired excretion can lead to hypermagnesemia.
Melatonin and autoimmune disorders: Melatonin can stimulate immune function and may theoretically worsen autoimmune conditions such as rheumatoid arthritis, lupus, or multiple sclerosis, though the clinical data are mixed.
Valerian withdrawal: Abrupt discontinuation after long-term high-dose use may cause rebound insomnia in some individuals, though this is less severe than benzodiazepine withdrawal.
Zinc and copper: Long-term zinc supplementation at doses above 30 mg can induce copper deficiency, which causes anemia and neurological symptoms.
Testing
If sleep supplements are not working, there may be an underlying physiological driver that needs to be identified rather than masked.
I use the following tests to assess sleep quality and root causes.
Blood And Urine Markers
Serum Ferritin: Low iron stores are strongly associated with Restless Leg Syndrome (RLS) and periodic limb movement disorder, both of which fragment sleep. R
Ferritin should be above 50-75 ng/mL in RLS patients, and above 100 ng/mL in severe cases.
I use the Foundation Zoomer (Vibrant Wellness) which includes ferritin, CBC, CMP, and thyroid markers in a single panel.
Vitamin D (25-OH): Vitamin D deficiency is associated with poor sleep quality, shorter sleep duration, and increased sleep latency. R
I use the Nutrient Zoomer (Vibrant Wellness) which includes vitamin D along with B6, B12, folate, zinc, copper, and magnesium.
Magnesium (RBC Magnesium): Serum magnesium is a poor reflection of total body magnesium status.
Red blood cell (RBC) magnesium is a better marker, and low RBC magnesium correlates with insomnia severity. R
The Nutrient Zoomer includes RBC magnesium.
Cortisol (Salivary, Diurnal): Blunted morning cortisol or elevated evening cortisol can drive sleep-onset or sleep-maintenance issues.
The Hormone Zoomer (Vibrant Wellness) includes a four-point salivary cortisol curve, DHEA, and melatonin metabolites.
Fasting Blood Glucose and Hemoglobin A1C: Nocturnal hypoglycemia is a common but overlooked cause of sleep-maintenance insomnia.
The Cardio Zoomer (Vibrant Wellness) includes fasting glucose, insulin, HOMA-IR, and HbA1C.
Homocysteine: Elevated homocysteine is associated with methylation cycle dysfunction and disrupted sleep architecture.
I use the Cellular Zoomer (Vibrant Wellness) for methylation markers including homocysteine.
Tryptase and Histamine: Mast cell activation can drive histamine-mediated insomnia, particularly in people with MCAS or histamine intolerance.
I use the Immune Zoomer (Vibrant Wellness) for mast cell and immune markers, and I also offer plasma histamine (Quest via Histamine, Plasma) and tryptase (Quest via Tryptase) through Fullscript.
Functional Lab Panels
When sleep issues are complex and accompanied by other chronic symptoms, I use comprehensive panels to assess root cause drivers.
I use the Gut Zoomer (Vibrant Wellness) to assess the gut microbiome, which directly regulates serotonin and GABA production.
I use the Mold Illness Bundle (Vibrant Wellness, includes Toxin + Immune + Neural Zoomers) when sleep issues accompany biotoxin illness symptoms such as fatigue, brain fog, and light sensitivity.
I use the Long COVID Bundle (Vibrant Wellness, includes Cardio + Toxin + Gut + Cellular + Viral Zoomers) for post-viral sleep disruption.
For comprehensive adrenal and hormonal assessment including the full circadian cortisol profile, I use the DUTCH Complete (Precision Analytical) through Fullscript.
Mechanisms Of Action
Simple
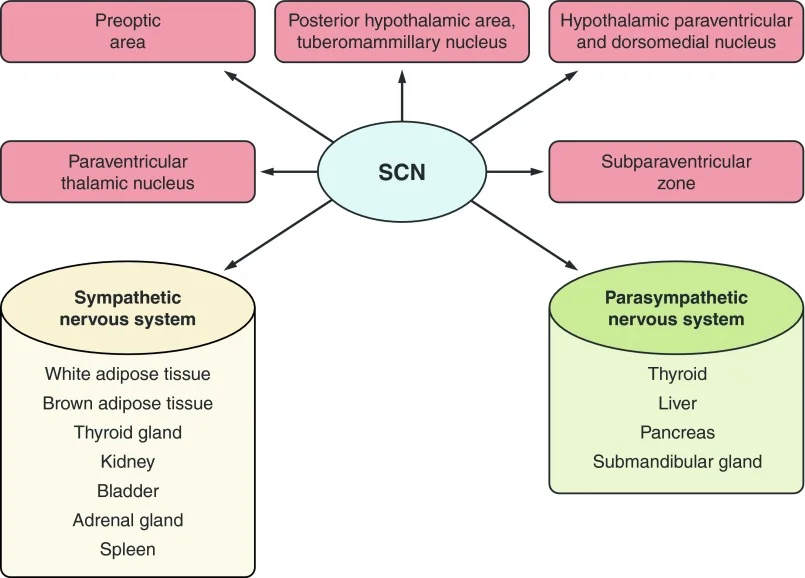
Melatonin binds to melatonin receptors in the brain's suprachiasmatic nucleus to signal that it is time to sleep.
Magnesium calms the nervous system by supporting GABA receptors and blocking the stress-excited NMDA receptors.
Glycine lowers core body temperature by dilating blood vessels, which tells the brain it is time to sleep.
L-theanine increases alpha brain waves, which are associated with a calm, meditative state.
Apigenin and valerian both boost GABA activity, which is the brain's primary brake pedal.
Ashwagandha and phosphatidylserine lower cortisol, the stress hormone that keeps you awake.
5-HTP provides the raw material for serotonin and then melatonin production.
Zinc helps regulate the balance between excitation and inhibition in the brain.
CBN interacts with the endocannabinoid system to reduce nighttime awakenings.
Ziziphus jujuba increases GABA receptor expression while also supporting brain growth factors.
Advanced
Melatonin (MTNR1A/MTNR1B agonism): Exogenous melatonin binds to high-affinity MT1 (MTNR1A) and MT2 (MTNR1B) receptors in the Suprachiasmatic Nucleus (SCN), phase-shifting the circadian clock and reducing sleep onset latency.
Low-dose (0.3-0.5 mg) produces physiological blood levels similar to endogenous nocturnal peaks, while high-dose (3-10 mg) produces supraphysiological levels that persist into the next morning and may cause phase delay rather than advance. R
Magnesium (NMDA antagonism, GABA-A cofactor): Magnesium ion (Mg2+) is a physiological antagonist of the NMDA glutamate receptor, blocking the calcium channel pore and reducing excitatory neurotransmission.
It also acts as a positive allosteric modulator of GABA-A receptors, increasing chloride ion conductance.
Magnesium is a cofactor for AANAT, the rate-limiting enzyme in melatonin synthesis. R
Glycine (NMDA co-agonist in SCN, thermoregulation): Glycine binds to the glycine-binding site on NMDA receptors in the SCN shell, activating a signaling cascade that increases cutaneous blood flow via nitric oxide-dependent vasodilation, dropping core body temperature by 0.2-0.5 degrees Celsius.
This temperature drop is necessary and sufficient for sleep onset.
SCN ablation completely abolishes the sleep-promoting and hypothermic effects of glycine. R
L-Theanine (alpha-wave enhancement, glutamate receptor modulation): L-theanine competitively inhibits glutamate binding to AMPA and kainate receptors, reducing cortical excitation.
It also increases brain levels of GABA, dopamine, and serotonin, and enhances alpha-band oscillatory activity (8-13 Hz) in the occipital and parietal cortex, which is the EEG signature of wakeful relaxation. R
Apigenin (GABA-A benzodiazepine site modulation, CD38 inhibition): Apigenin binds to the benzodiazepine site on GABA-A receptors with a Ki of approximately 4 microM, producing anxiolytic and sedative effects without the muscle relaxation or tolerance seen with classical benzodiazepines.
It also inhibits CD38, an NADase that degrades NAD+, potentially increasing NAD+ levels and supporting sirtuin activity. R
Ashwagandha (HPA axis modulation, GABA-A positive modulation): The withanolides in ashwagandha, particularly Withaferin A and Withanolide D, modulate the HPA axis by reducing CRH and ACTH signaling, which downregulates cortisol synthesis in the adrenal cortex.
Ashwagandha also acts as a positive allosteric modulator of GABA-A receptors and increases GAD65/67 expression, the enzymes that synthesize GABA. R
Phosphatidylserine (cortisol blunting, ACTH suppression): PS suppresses ACTH release from the pituitary gland in response to CRH, attenuating the cortisol response to physical and psychological stress.
It also incorporates into neuronal membranes and supports protein kinase C signaling, which is involved in neurotransmitter release and synaptic plasticity. R
CBN (CB1 partial agonist, sedation): CBN is a partial agonist at CB1 receptors with approximately 10-25% of the potency of THC.
It also activates TRPA1 and TRPV2 channels and inhibits FAAH, increasing endocannabinoid tone.
Unlike THC, CBN does not produce significant psychoactive effects at moderate doses. R
Zinc (NMDA modulation, GABA-A potentiation): Zinc is stored in synaptic vesicles of glutamatergic neurons and co-released with glutamate, where it modulates NMDA and GABA-A receptors.
Zinc potentiates GABA-A receptor-mediated currents at low concentrations and inhibits NMDA receptors by binding to an allosteric site on the NR2A subunit. R
Ziziphus Jujuba (GABA-A upregulation, BDNF induction, 5-HT modulation): Saponins (jujubosides) and flavonoids from Ziziphus spinosa seeds upregulate GABA-A receptor expression and inhibit serotonin (5-HT) degradation, increasing synaptic 5-HT availability.
The triterpenoid betulinic acid activates NRF2 signaling, while jujuboside A increases BDNF, GDNF, and NT-3 expression via the ERK/CREB pathway. R
Genetics
MTNR1B
The MTNR1B gene encodes the melatonin receptor MT2, which mediates the phase-shifting effects of melatonin on the circadian clock.
The rs10830963 risk variant (G allele) is associated with impaired melatonin signaling, higher fasting glucose, and increased diabetes risk. R
Carriers of this variant may require higher or differently timed melatonin doses to achieve the same circadian phase shift.
COMT
The Catechol-O-Methyltransferase (COMT) gene encodes the enzyme that breaks down dopamine, norepinephrine, and estrogen.
The Val158Met (rs4680) polymorphism determines enzyme activity.
Met/Met carriers (low activity) have higher baseline dopamine and are more sensitive to stress, often with better response to L-theanine and magnesium for sleep.
Val/Val carriers (high activity) break down dopamine rapidly and may have lower pain tolerance and more sleep disruption from stress.
SLC6A4 (5-HTTLPR)
The Serotonin Transporter gene (SLC6A4) has a functional polymorphism (5-HTTLPR) with short (S) and long (L) alleles.
S-allele carriers have reduced serotonin transporter function, lower serotonin reuptake, and higher risk of insomnia and stress sensitivity. R
Carriers of the S-allele may derive greater benefit from tryptophan or 5-HTP supplementation, as a 2019 crossover trial found marginally significant improvements in subjective sleep quality specifically in S-allele carriers. R
GABRA1 / GABRA2
Variants in the GABA-A receptor subunit alpha 1 and 2 genes (GABRA1, GABRA2) influence benzodiazepine sensitivity and baseline GABAergic tone.
Individuals with hypofunctional GABA-A variants may respond better to apigenin, valerian, or magnesium glycinate, all of which enhance GABAergic signaling through different mechanisms.
BHMT / MTHFR
Betaine-Homocysteine S-Methyltransferase (BHMT) and Methylenetetrahydrofolate Reductase (MTHFR) variants affect methylation cycle efficiency, which impacts melatonin and neurotransmitter synthesis.
Impaired methylation reduces the conversion of 5-HTP to serotonin and serotonin to melatonin, which may explain why some people with MTHFR variants have treatment-resistant insomnia that responds to methylated B-vitamin support.
More Research
Acute vs Chronic Effects: Most sleep supplement studies are short-term (1-12 weeks), and we need more data on long-term efficacy, tolerance, and safety.
The exception is melatonin, which has been studied for years to decades in shift workers and certain populations without evidence of tolerance at low doses.
Objective vs Subjective Sleep Measures: Many supplements improve subjective sleep quality (how well you feel you slept) without changing objective sleep architecture (polysomnography).
Valerian is a classic example: consistent subjective benefit but inconsistent objective changes.
This does not mean the supplements are useless, but it does mean we cannot always trust the feeling of good sleep as the complete picture.
Nutrient-Gene Interactions: The emerging field of nutrigenomics suggests that individual responses to sleep supplements may be strongly influenced by genetic variants in neurotransmitter and methylation pathways.
For example, the 5-HTTLPR S-allele carriers derive more sleep benefit from tryptophan than L-allele carriers. R
Melatonin Beyond Sleep: Melatonin is a potent antioxidant and anti-inflammatory compound, and its effects on NRF2, NF-kB, and mitochondrial function may be as important as its sleep-regulating effects for overall health. R
The Combination Gap: Most clinical trials test single agents, but patients rarely use them that way.
The safety of long-term combination therapy is not well studied, and potential interactions between sleep supplements and prescription medications are under-researched.
Glymphatic Clearance: Deep sleep is when the glymphatic system clears amyloid-beta and tau proteins from the brain.
Supplements that increase slow-wave sleep (glycine, magnesium, delta-inducing agents) may therefore have neuroprotective effects that go far beyond sleep quality.
I covered this in improve glymphatic system and AQP4 biohacks.
Magnesium and Glycine Synergy: Magnesium glycinate provides both magnesium and glycine, but the glycine dose per serving (approximately 200-500 mg) is far below the 3 g needed for the thermoregulatory sleep mechanism.
A separate glycine supplement may be needed in addition to magnesium glycinate if the thermoregulatory effect is the goal.
For biomarker testing I use the Nutrient Zoomer (Vibrant Wellness) to assess magnesium, zinc, copper, and B-vitamin status, the Cellular Zoomer to assess methylation and oxidative stress markers, and the Hormone Zoomer to assess the diurnal cortisol rhythm.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Lion's Mane
1000mg/day
Omega-3 (DHA)
2g/day
Phosphatidylserine
100mg 3x/day