Endometriosis: Inflammation, Estrogen, and Immune Dysfunction Beyond "Misplaced Tissue"
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Endometriosis is usually described as endometrial tissue growing in the wrong place, but that framing misses what actually drives the pain, the lesion growth, and the recurrence after surgery.
In this post, we will discuss why endometriosis is better understood as an inflammatory and immune disease, how lesions manufacture their own estrogen, why mast cells and macrophages amplify pain, which environmental exposures raise risk, and an evidence-based approach to lowering the inflammatory load.

Basics Of Endometriosis
Endometriosis is a chronic condition in which tissue resembling the uterine lining grows outside the uterus, most often on the ovaries, the pelvic peritoneum, and the deep pelvic structures.
It affects roughly 10% of reproductive-age women.
The classic explanation is retrograde menstruation, the backward flow of menstrual debris through the fallopian tubes into the pelvic cavity, where cells implant and grow.
The problem with stopping there is simple.
Retrograde menstruation happens in most menstruating women, yet only about one in ten develops endometriosis. R
So the interesting question is not how the cells arrive, it is why the immune system fails to clear them and why the tissue that survives behaves so aggressively.
The current view frames endometriosis as an estrogen-dependent chronic inflammatory disease with significant immune dysfunction, not a simple mechanical accident. R R
This matters for treatment.
If the disease is driven by local estrogen production, immune escape, and neuroinflammation, then surgery alone rarely fixes the underlying terrain.
What Causes Endometriosis
Endometriosis is not caused by one thing.
It emerges when seeding, hormones, immune failure, and environmental load stack together.
Root contributors (not an exclusive list):
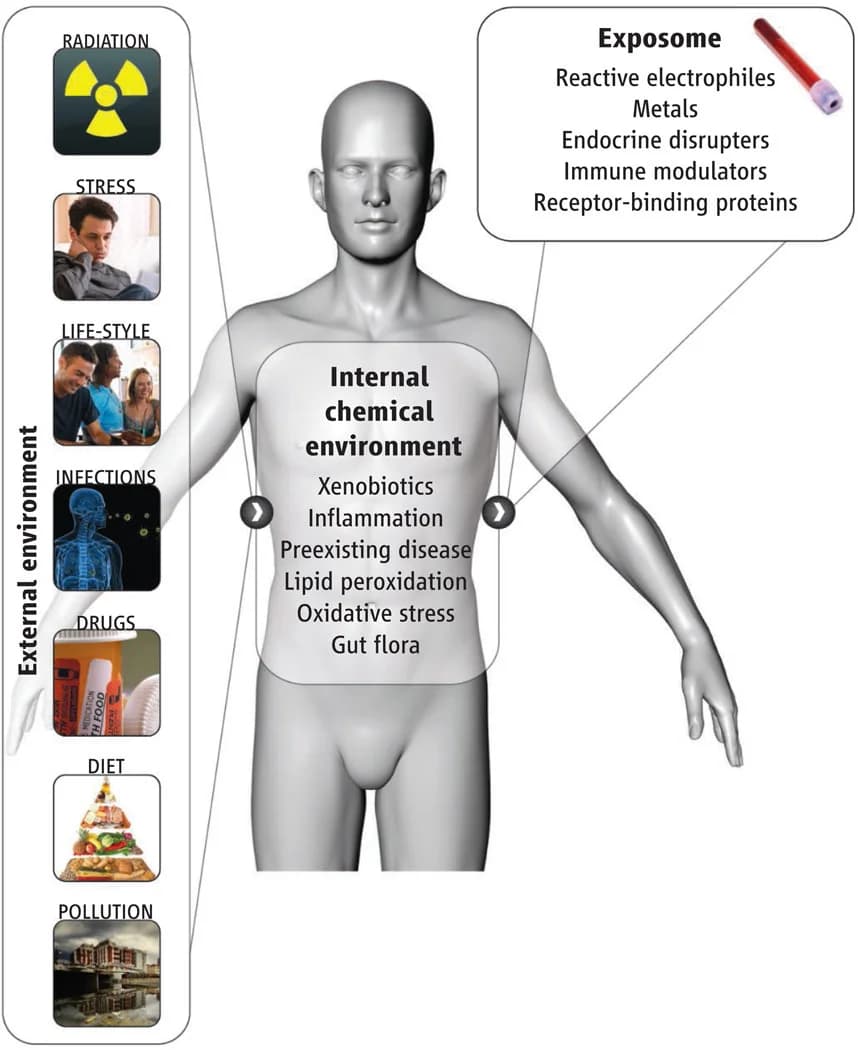
- Environmental endocrine disruptors (dioxins, PCBs, BPA, and phthalates are associated with higher prevalence) R
- Genetic susceptibility (over 40 risk loci, many in estrogen-signaling genes) R
- Immune dysfunction (impaired natural killer cell clearance of ectopic tissue) R
- Local estrogen synthesis (lesions make their own estradiol) R
- Progesterone resistance (the brake on estrogen and inflammation stops working) R
- Retrograde menstruation (the seeding event, necessary but not sufficient) R
The most useful way to read this list is as a permission problem.
Retrograde menstruation seeds the cells, but genetic makeup, hormonal environment, and toxic exposures decide whether those cells survive, and immune dysfunction is the permissive factor that lets them evade clearance and vascularize. R
The Immune Failure
In healthy immune surveillance, natural killer cells and macrophages recognize and destroy stray endometrial fragments before they can implant.
In endometriosis, natural killer (NK) cell cytotoxicity is measurably reduced in both blood and peritoneal fluid. R
The lesions also build an actively immunosuppressive microenvironment.
High local levels of Transforming Growth Factor Beta (TGF-β), Interleukin-6 (IL-6), and Interleukin-10 (IL-10) blunt NK killing and let ectopic tissue persist. R
Macrophages, which should be clearing debris, are reprogrammed into a wound-healing phenotype that instead feeds the lesion with growth factors and new blood vessels. R
This is why the disease looks less like misplaced tissue and more like a chronic, self-sustaining inflammatory lesion that the immune system has been talked into protecting.

How Endometriosis Lesions Create Their Own Estrogen
This is the mechanistic core, and it is the part most patients are never told.
Normal endometrium cannot synthesize estrogen because it lacks the enzyme aromatase.
Endometriotic lesions are different.
They express aromatase (CYP19A1) and Steroidogenic Acute Regulatory protein (StAR), which lets them build estradiol from cholesterol right inside the lesion. R
They also carry a second defect in estrogen metabolism.
The enzyme 17-beta-Hydroxysteroid Dehydrogenase type 1 (17β-HSD1), which converts weak estrone into potent estradiol, is overactive in lesions, while the type 2 enzyme that would deactivate estradiol back to estrone is deficient. R
The result is a local estradiol trap.
Lesions crank up estradiol production and simultaneously fail to break it down, so the tissue marinates in the exact hormone that drives its growth. R
Estradiol then stimulates prostaglandin E2 (PGE2), and PGE2 in turn stimulates more aromatase, creating a feed-forward loop of estrogen and inflammation that does not need the ovaries to keep running.
Progesterone Cannot Apply The Brake
Progesterone normally opposes estrogen and calms the endometrium.
In endometriosis, the tissue is progesterone resistant, with reduced expression of the progesterone receptor, especially the PR-B form. R
The practical consequence is that estrogen dominates unopposed, inflammation stays elevated, and about a third of women get inadequate relief from progestin-based therapy. R
If you want the upstream picture of how estrogen and progesterone are supposed to balance, see the female hormone pathway and the work of Felice Gersh on estrogen receptors.
Endometriosis And Overlapping Conditions
Endometriosis rarely travels alone, and the overlaps point back to the same inflammatory and immune terrain.
Mast Cells And Pain
Mast cells are dramatically enriched in endometriotic lesions, and far more of them are degranulated compared to normal endometrium. R
These mast cells cluster next to nerve fibers.
When they degranulate, they release histamine, tryptase, and Nerve Growth Factor (NGF), which sprouts new pain-sensing nerve fibers into the lesion and lowers their firing threshold. R
Newer work maps a specific pathway, in which mast cell activation through the MRGPRX2 receptor sensitizes sensory neurons via histamine acting on HRH1 and TRPV1 channels. R
Estrogen makes this worse, because it primes mast cells to release more of their contents, tying the hormonal and neuroimmune sides of the disease together. R
This is why women with endometriosis often also carry features of mast cell overactivity.
If histamine symptoms, flushing, or reactivity track with your cycle, the overlap with mast cell activation syndrome is worth understanding, and the broader biology of mast cells is covered separately.
Other Overlaps
- Autoimmune conditions (endometriosis clusters with immune-mediated disease, consistent with its immune dysfunction) R
- Estrogen-driven conditions (the same estrogen-receptor biology that drives endometriosis overlaps with other estrogen receptor and xenoestrogen conditions)
- Pelvic pain and dysautonomia (chronic pain and autonomic symptoms can co-travel, and some readers will also be tracking POTS)
How To Improve Endometriosis
Nothing here replaces surgical or gynecologic care for a disease that can damage organs and fertility.
The goal of this section is to lower the inflammatory and estrogenic load that keeps lesions active, alongside proper medical management.
1. Anti-Inflammatory, Lower-Estrogen Diet
This is the highest-leverage lever with real prospective data behind it.
In 12 years of Nurses' Health Study II data, women eating the most long-chain omega-3 fats were 22% less likely to be diagnosed with endometriosis, while those eating the most trans fats were 48% more likely. R
Practical translation.
Increase oily fish and other omega-3 sources, and eliminate industrial trans fats entirely.
Emphasize fiber, because fiber supports estrogen clearance through the gut, and reduce alcohol, which raises estrogen and burdens the liver.
2. Omega-3 Fatty Acids
Fish Oil: Omega-3 intake is associated with reduced pain and lower inflammatory cytokines in endometriosis, shifting eicosanoid production away from the pro-inflammatory arachidonic acid pathway. R
The evidence is mixed on lesion size but reasonably consistent on pain, and the safety profile is excellent.
3. N-Acetylcysteine
N-Acetylcysteine: In a clinical study, oral NAC dosed at 600 mg three times daily for three consecutive days per week over three months reduced endometriosis-related pain, shrank endometriomas, and lowered CA-125. R
NAC is one of the few supplements here with human lesion data rather than only animal data, and it doubles as a glutathione precursor for antioxidant support.
4. Green Tea Catechins
EGCG: Green tea epigallocatechin gallate (EGCG) inhibits lesion angiogenesis in animal models by suppressing VEGF-C and VEGFR2 signaling, which lesions depend on for blood supply. R
This is animal-model evidence, and standard EGCG has poor bioavailability, so treat it as a supportive anti-angiogenic rather than a proven therapy.
Endometriosis is an angiogenesis-dependent disease, which is worth understanding alongside the broader role of VEGF.
5. Curcumin And Resveratrol
Curcumin: Curcumin reduces lesion size and growth rate in animal models, though human trials are small and mixed. R
Resveratrol: Resveratrol has anti-inflammatory and anti-estrogenic activity in preclinical work, but human evidence as a standalone agent is not yet convincing. R
There is a big MAYBE with both of these.
Use them as anti-inflammatory support, not as the load-bearing part of a protocol.
6. Support Estrogen Clearance And Gut Health
A meaningful fraction of your estrogen is recirculated through the gut.
Support the microbes and the liver conjugation pathways that package estrogen for excretion, keep bowels regular with fiber, and address any dysbiosis that raises reabsorption.
Magnesium is reasonable for cramping and general smooth-muscle relaxation, and Magnesium Glycinate is a well-tolerated form.
7. Reduce Environmental Estrogen Exposure
This is covered in the next section, and it is not optional given the toxicant data.
What To Stay Away From
Exposures and inputs to reduce (not an exclusive list):
- Alcohol (raises circulating estrogen and adds liver burden)
- BPA and BPS plastics (bisphenols are associated with endometriosis and act as xenoestrogens) R
- Dioxins and PCBs (persistent organochlorines associated with higher endometriosis prevalence and altered estrogen-receptor signaling) R
- Phthalates (plasticizers in fragrance, soft plastics, and personal care are associated with the disease) R
- Trans fats (highest intake linked to 48% higher diagnosis risk) R
The organochlorine and plastics data are the reason environmental load belongs in any serious endometriosis conversation.
These compounds are covered in depth in the posts on xenoestrogens and estrogenics and on phthalates specifically.
The practical moves are unglamorous and effective.
Stop heating food in plastic, filter your water, switch to fragrance-free personal care, and avoid handling thermal receipts.
Testing
Endometriosis is definitively diagnosed by laparoscopy with biopsy, not by a blood test.
The labs below do not diagnose the disease, they assess the hormonal, inflammatory, and toxic terrain that drives it, which is where an at-home lab workup adds value.
Imaging And Diagnosis
Transvaginal ultrasound and MRI can detect endometriomas and deep infiltrating lesions, but superficial peritoneal disease is often invisible on imaging and only confirmed surgically.
Blood Markers
CA-125 is frequently elevated in endometriosis, but it is nonspecific and unreliable, since it also rises with menstruation, fibroids, pelvic infection, and ovarian pathology, so it is best used to track change over time rather than to rule the disease in or out. R
For hormonal context I use the Hormone Zoomer (Vibrant Wellness) to assess estradiol, progesterone, and estrogen metabolism, or the DUTCH Complete (Precision Analytical) when I want detailed estrogen-metabolite pathways.
Individual markers are also available, including Estradiol (Quest Diagnostics) and Progesterone (Quest Diagnostics), timed to the luteal phase.
Functional Lab Panels
I use the Immune Zoomer (Vibrant Wellness) to assess autoantibodies and immune reactivity given the immune-dysfunction basis of the disease.
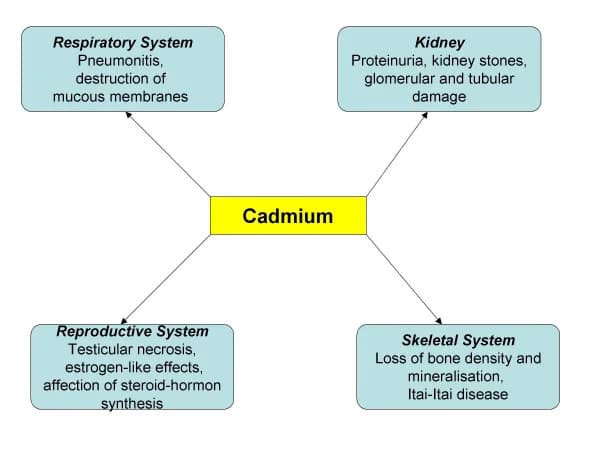
I use the Toxin Zoomer (Vibrant Wellness) to assess environmental chemical and heavy-metal load, which is directly relevant given the organochlorine and phthalate data.
For estrogen recirculation and gut health I use the Gut Zoomer (Vibrant Wellness) or the GI-MAP (Diagnostic Solutions), which reflect the microbial side of estrogen clearance.
Vitamin D status is worth checking with the Nutrient Zoomer (Vibrant Wellness) or a standalone Vitamin D, 25-Hydroxy (Quest Diagnostics), since low vitamin D is common in inflammatory disease.
If you want help interpreting a full panel against your symptoms, that is exactly what a consultation is for.

Mechanisms Of Action
Simple:
- Endometriosis lesions build their own estrogen and cannot switch it off, so they keep growing even away from the ovaries.
- The immune system that should be clearing the stray tissue is suppressed, and mast cells near the lesions release chemicals that grow new nerves and amplify pain.
Advanced:
- Local steroidogenesis Lesions ectopically express StAR and aromatase (CYP19A1), enabling de novo estradiol synthesis from cholesterol that eutopic endometrium cannot perform. R
- Estradiol trapping Elevated 17β-HSD type 1 converts estrone to estradiol while deficient type 2 fails to inactivate it, and estradiol drives PGE2 via COX-2, which feeds back to further induce aromatase in a self-amplifying loop. R
- Progesterone resistance Downregulation of the progesterone receptor, particularly PR-B, removes the antiestrogenic and anti-inflammatory brake, sustaining proliferation and inflammatory signaling. R
- Impaired immune clearance Reduced NK cytotoxicity, driven by a dysregulated activating-inhibitory receptor balance and immunosuppressive TGF-β, IL-6, and IL-10, allows ectopic implants to evade lysis. R
- Neuroangiogenesis and mast cell sensitization Lesion-resident mast cells and M2 macrophages secrete NGF and VEGF, driving nerve sprouting and vascularization, while MRGPRX2-mediated mast cell degranulation sensitizes nociceptors through histamine, HRH1, and TRPV1. R
Genetics
Genome-wide association studies have identified more than 40 endometriosis risk loci, and many sit in genes that control estrogen signaling and reproductive-tract development. R
WNT4
WNT4 encodes a signaling protein essential for female reproductive tract development and ovarian function.
Variants alter Müllerian duct and endometrial development.
rs7521902 is one of the most consistently replicated endometriosis risk variants across populations. R
GREB1
GREB1 encodes an early estrogen-response gene that acts as a growth regulator in estrogen signaling.
Variants increase estrogen-driven proliferative signaling.
rs13394619 is associated with endometriosis susceptibility. R
CYP19A1
CYP19A1 encodes aromatase, the enzyme that converts androgens into estrogens.
Because lesions ectopically express this enzyme, variation here is mechanistically central to local estrogen production.
CYP19A1 has been identified as an endometriosis-associated locus involved in sex-steroid regulation. R
ESR1 And ESR2
ESR1 and ESR2 encode estrogen receptor alpha and beta.
In endometriosis, estrogen receptor beta is strikingly overexpressed in lesions and reshapes inflammatory and apoptotic signaling.
Variants in both receptor genes are associated with susceptibility. R
More Research
- Aromatase inhibitors, which block the lesion's own estrogen factory, are an active area of research for estrogen that persists despite ovarian suppression, and they illustrate why the local-synthesis model matters clinically. R
- Endocrine-disrupting chemical exposure remains a strong and biologically plausible association across most published studies, though causation in humans is difficult to prove because exposures are chronic, mixed, and hard to measure. R
- For biomarker testing I use the Hormone Zoomer and the Toxin Zoomer together, because the disease sits at the intersection of estrogen biology and environmental load.
- Progesterone resistance explains a real clinical frustration, that standard progestin therapy fails in roughly a third of women, and it argues for addressing inflammation and estrogen metabolism upstream rather than relying on hormonal suppression alone. R
- The mast cell and neuroangiogenesis story is the most promising frontier for pain that persists after lesions are surgically removed, since the sensitized nerves and the neuroimmune loop do not necessarily leave with the tissue. R
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Quercetin
500mg 2x/day
Vitamin D3 + K2
5000 IU + 200mcg/day
DAO Enzyme
1 cap before meals