8 Steps to Naturally Treat Mold Illness And CIRS (Science-Based Protocol)
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
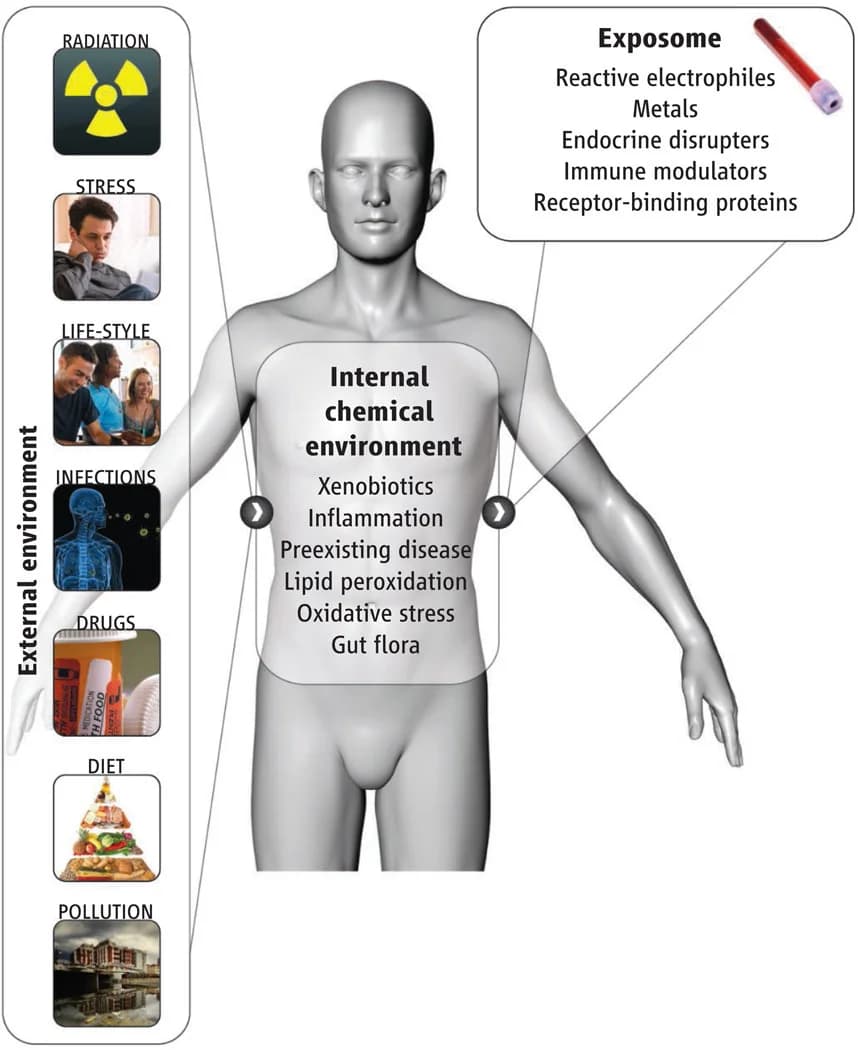
Mold illness is what happens when biotoxins from a water-damaged building trigger a chronic immune activation that does not switch off after you leave the building.
In this post, we will discuss what mold illness and CIRS actually are, why I think the standard model gets the mechanism backwards, how mold drives illness through Junction Dysfunction, the protocol I use, and how to test for it without falling for unvalidated lab marketing.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Quercetin
500mg 2x/day
Vitamin D3 + K2
5000 IU + 200mcg/day
DAO Enzyme
1 cap before meals