Aminophenazone (Aminopyrine): The Analgesic That Was Pulled From Markets Worldwide
By Jacob Gordon, INHC, FMT-CAminophenazone goes by several names depending on the era and country: aminopyrine, amidopyrine, dimethylaminoantipyrine, and its trade name Pyramidon. R
It was one of the most widely used analgesics in the first half of the twentieth century. R
It is now banned or withdrawn from clinical use in the United States, France, Japan, India, Thailand, and most other developed nations. R
This post covers what aminophenazone is, how it works, why it was withdrawn, what its remaining scientific uses are, and what it tells us about drug safety history.
This is not a post about a supplement, peptide, or optimization compound.
Aminophenazone is a pharmaceutical with a well-documented and serious toxicity profile.
It is included here as a reference compound with pharmacological relevance to understanding COX inhibition, drug-induced agranulocytosis, and liver function testing.
What Aminophenazone Is
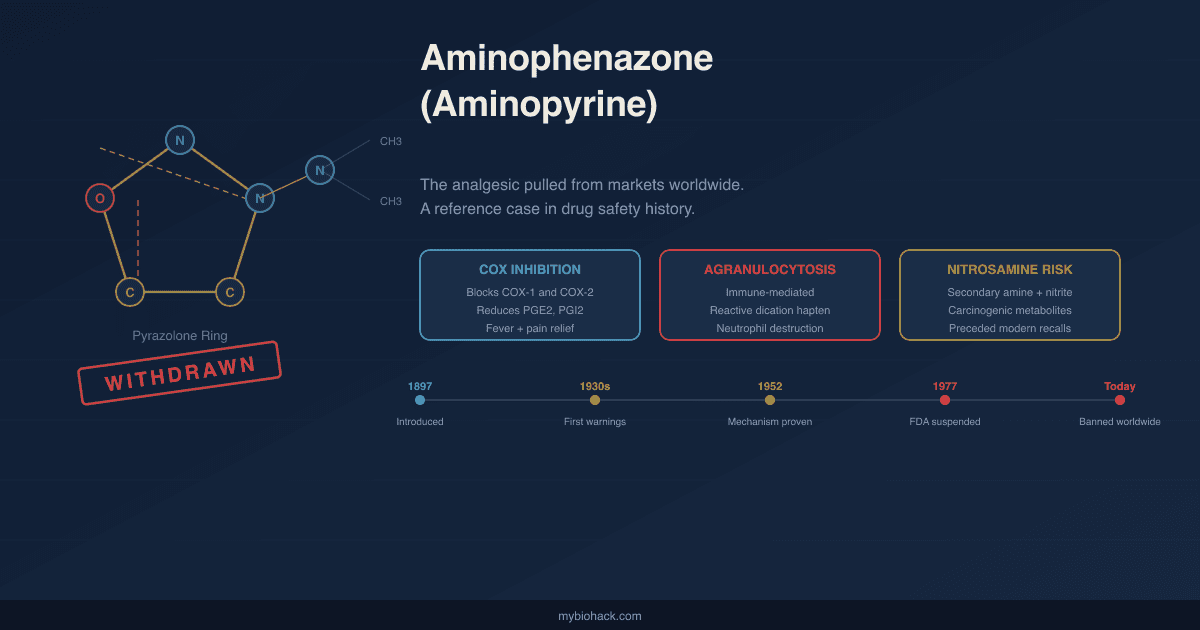
Chemical class: Pyrazolone derivative
Molecular formula: C₁₃H₁₇N₃O
Also known as: Aminopyrine, amidopyrine, dimethylaminoantipyrine, 4-dimethylaminoantipyrine
Trade name: Pyramidon (Hoechst AG)
CAS number: 58-15-1
Melting point: 107 to 109°C R
Aminophenazone is a synthetic non-narcotic analgesic, antipyretic, and mild anti-inflammatory agent. R
It belongs to the pyrazolone chemical class, a family of five-membered heterocyclic lactam compounds also including phenazone (antipyrine), propyphenazone, and metamizole (dipyrone). R
Origin and synthesis:
The pyrazolone chemistry began in 1883 when Ludwig Knorr synthesized phenazone (antipyrine) by condensing phenylhydrazine with ethyl acetoacetate, producing the first commercially successful synthetic analgesic and antipyretic. R
Phenazone was introduced into clinical practice in 1884. R
Aminophenazone was first synthesized in 1893 by Friedrich Stolz at Farbwerke Hoechst as a structural derivative of phenazone. R
The synthesis introduced a dimethylamino group at the 4-position of the pyrazolone ring: phenazone is nitrosated with sodium nitrite in sulfuric acid to give 4-nitroso-antipyrine, reduced to 4-aminoantipyrine (the primary active metabolite), then subjected to reductive methylation via the Eschweiler-Clarke reaction using formaldehyde and formic acid to yield the dimethylamine. R
This industrial route achieves 70 to 80% overall yield after recrystallization from ethanol. R
The modification produced a compound with faster onset, lower required doses, and superior analgesic potency compared to phenazone. R
By 1896, preliminary human trials confirmed efficacy for fever, headache, and rheumatic pain. R
Hoechst patented and commercialized it as Pyramidon in 1897. R
Physical properties:
Aminophenazone appears as white leaf-like crystals or crystalline powder with no significant odor and a slightly bitter taste. R
It is stable in air but deteriorates on exposure to sunlight and is readily attacked by mild oxidizing agents in the presence of water. R
It is soluble in water (aqueous solutions are weakly alkaline, pH 7.5 to 9), alcohol, chloroform, benzene, and ether. R
Pharmacological properties:
Aminophenazone is water-soluble and well-absorbed after oral administration with rapid onset of action. R
It was used at doses of 300 to 500 mg for analgesia and fever reduction, typically two to three times daily. R
Its analgesic potency was considered greater than aspirin for equivalent doses in the conditions it was most used to treat: rheumatism, neuritis, and migraine. R
Gastrotoxicity was less common than with other analgesic and anti-inflammatory drugs, probably because of its weaker anti-inflammatory effect relative to prostaglandin suppression in the gastric mucosa. R
Mechanism Of Action
COX inhibition:
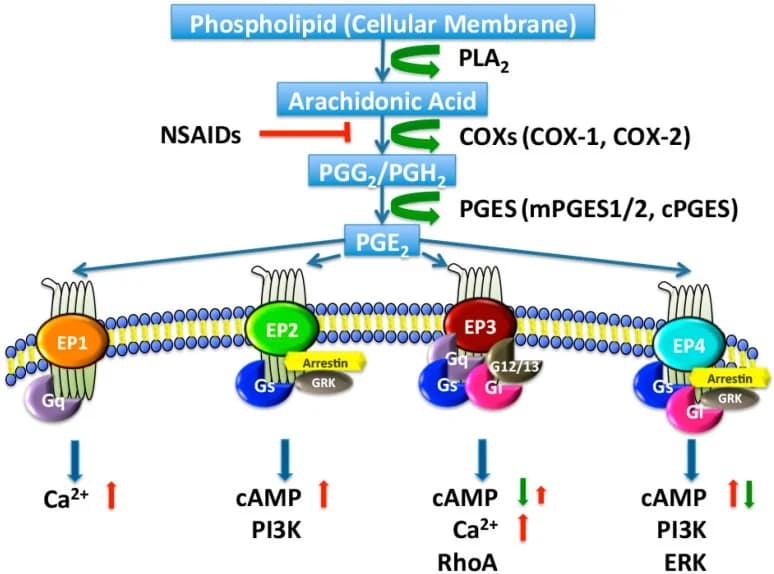
Aminophenazone's primary mechanism is inhibition of cyclooxygenase (COX) enzymes, specifically both COX-1 and COX-2. R
COX enzymes catalyze the conversion of arachidonic acid to prostaglandin H₂ (PGH₂), the unstable precursor from which all prostaglandins and thromboxanes are synthesized. R
By blocking this step, aminophenazone reduces prostaglandin E₂ (PGE₂) and prostaglandin I₂ (PGI₂), the primary mediators of fever, nociceptor sensitization, and tissue inflammation. R
The drug also inhibits rat gastric mucosal 6-keto-prostaglandin F1 alpha production with an IC₅₀ of 3.8 × 10⁻³ M, confirming direct prostaglandin biosynthesis inhibition. R
Antipyretic mechanism:
The antipyretic action involves reducing PGE₂ synthesis in the hypothalamus, where PGE₂ acts on EP3 receptors to raise the thermoregulatory set point during fever. R
Blocking hypothalamic PGE₂ synthesis resets the elevated set point back toward normal, reducing core temperature without impairing normal thermoregulation. R
Central analgesic mechanism: descending inhibition via the PAG:
Beyond peripheral COX inhibition, aminophenazone produces central antinociception by activating descending inhibitory pathways originating in the periaqueductal gray (PAG). R
The PAG is a midbrain structure that forms the primary hub of endogenous pain modulation, projecting via the rostroventromedial medulla (RVM) to the spinal cord dorsal horn to inhibit ascending nociceptive transmission. R
In rats, microinjection of procaine into the PAG abolished the antinociceptive effect of systemically administered aminophenazone (150 mg/kg), confirming that intact PAG function is required for the drug's central analgesic action. R
The same procaine block did not significantly reduce the antinociception produced by threshold doses of morphine, indicating that aminophenazone's PAG-mediated mechanism overlaps with but is not identical to opioid-mediated descending inhibition. R
This is consistent with a class effect across pyrazolones: dipyrone and related compounds induce antinociception through a PAG-RVM-spinal cord axis that operates independently of direct opioid receptor agonism. R
Anti-inflammatory effect:
Aminophenazone's anti-inflammatory effect is described as weaker than other NSAIDs, which may explain the relatively lower gastrotoxicity compared to aspirin or indomethacin. R
Additional mechanisms:
Some studies suggest involvement of COX-3 (a splice variant of COX-1 expressed primarily in the central nervous system) in the actions of pyrazolone-class drugs, though the pharmacological relevance of COX-3 as a distinct target remains controversial. R
The primary active metabolite 4-aminoantipyrine retains similar COX-inhibitory activity to the parent compound and extends the duration of action beyond what aminophenazone's own plasma half-life predicts. R
Overdose toxidrome:
In overdose, aminophenazone mainly affects the central nervous system, causing coma and convulsions, and damages the liver. R
Fatal intoxication has occurred in infants at lower doses than those causing toxicity in adults. R
Pharmacokinetics And Metabolism
Absorption:
Rapid and complete after oral administration; well-absorbed from the gastrointestinal tract. R
Distribution:
Aminophenazone distributes widely and evenly throughout body water compartments. R
This property has been exploited in research: aminophenazone has been used as a dilution marker to measure total body water in humans. R
Metabolism:
Aminophenazone is extensively metabolized in the liver through the cytochrome P450 (CYP) microsomal enzyme system. R
The dominant pathway is stepwise N-demethylation of the dimethylamino group. R
The CYP isoforms responsible include CYP1A2, CYP2C19, CYP2D6, CYP3A4, and CYP2C18. R
Principal metabolites include: R
- 4-Aminoantipyrine: the primary pharmacologically active metabolite, retaining analgesic and antipyretic activity
- Monomethylaminoantipyrine: the demethylation intermediate
- Rubazoic acid: produces reddish urine discoloration at high doses
- Methylrubazoic acid: also reddish; historically served as a dosing marker
At high doses, the presence of rubazoic acid and methylrubazoic acid in urine produces a characteristic reddish-brown discoloration that historically alerted clinicians to aminophenazone use. R
Half-life and elimination:
Plasma half-life is approximately 2 to 4 hours for aminophenazone itself, extended by the active metabolite 4-aminoantipyrine. R
Demethylation is the major elimination pathway; a significant alternative non-demethylation route also exists for the monomethyl intermediate. R
Critically, only approximately 50% of labeled carbon generated by N-demethylation is eventually oxidized all the way to CO₂ and exhaled; the remainder enters intermediary carbon metabolism. R
This is why aminopyrine breath test recoveries are expressed as a percentage of the administered dose rather than as an absolute rate. R
Metabolism in liver disease is significantly impaired, making the N-demethylation rate a sensitive readout of functional hepatic CYP450 microsomal mass. R
This property became the basis of the aminopyrine breath test, discussed below.
CYP2C19 polymorphism effect:
CYP2C19 is a principal enzyme in aminophenazone N-demethylation and a clinically important genetic determinant of aminopyrine breath test values. R
Poor metabolizers (two loss-of-function CYP2C19 alleles) clear aminophenazone more slowly, producing falsely low breath test values that can mimic hepatic dysfunction even in metabolically healthy individuals. R
This pharmacogenomic confounder must be considered when interpreting breath test results across diverse populations. R
Metabolism is also abnormally slow in newborns due to immature CYP450 systems; older infants show progressively higher ¹³CO₂ exhalation as microsomal capacity matures. R
Drug interactions:
Aminophenazone is a broad CYP450 substrate subject to induction and inhibition by other drugs. R
Phenobarbitone and other enzyme-inducing drugs increase aminophenazone clearance, raising breath test values above the normal range. R
Oral contraceptive steroids markedly inhibit aminophenazone metabolism: cumulative ¹³CO₂ percent dose recovery at day 21 of the menstrual cycle averaged 6.1 ± 2.3% in oral contraceptive users versus 12.1 ± 1.6% in non-users, an approximately 50% reduction. R
This effect reversed to near-normal values (10.2 ± 3.5%) within 7 days of stopping oral contraceptive steroid use. R
Cigarette smoking induces CYP1A2 and raises aminophenazone clearance; the combined effect of smoking and oral contraceptive steroid use results in approximately unchanged overall metabolic activity due to opposing CYP induction and inhibition. R
Historical Use
Aminophenazone's clinical history spans roughly eight decades, from commercial introduction in 1897 to withdrawal in most developed countries between the 1960s and 1990s. R
Peak use era:
Aminophenazone was among the most prescribed analgesics and antipyretics in Europe, Japan, and North America during the first half of the twentieth century. R
Approved uses included acute rheumatism, arthritis, neuralgia, neuritis, migraine (often in combination with ergotamine and caffeine), myositis, and chorea. R
In cases of prolonged intractable fever such as in Hodgkin's disease and periarteritis nodosa, aminopyrine was sometimes the only drug capable of controlling fever, though expert guidance at the time already cautioned it should only be used with proper supervision and monitoring when safer alternatives had failed. R
It was inexpensive, rapidly effective, had good oral bioavailability, and produced reliable results at consistent doses. R
Its analgesic potency per milligram compared favorably to aspirin for rheumatological conditions without aspirin's significant GI bleeding risk. R
First signals of danger:
Agranulocytosis reports began appearing in the medical literature in the 1930s. R
A 1936 JAMA report documented leukopenia in patients receiving an aminopyrine-containing preparation, noting that the medical profession was already reducing prescribing because of this danger. R
In Denmark, which maintained comprehensive pharmacy surveillance data, agranulocytosis cases and deaths attributable to aminopyrine were systematically tracked through the 1950s and 1960s. R
The landmark 1952 study by Moeschlin and Wagner established the immune-mediated mechanism when an investigator injected himself with serum from a patient with aminopyrine-induced agranulocytosis and experienced an immediate and precipitous drop in his neutrophil count, providing the first definitive demonstration of drug-dependent anti-neutrophil antibodies in medical history. R
Why It Was Withdrawn: Agranulocytosis
Agranulocytosis is defined as a peripheral neutrophil count below 500 cells per microliter. R
At this level, innate immune defense against bacterial and fungal pathogens collapses and even routine commensal organisms become potentially fatal. R
Aminophenazone is the prototype drug for immune-mediated agranulocytosis, and its mechanism is among the best-characterized of any drug-induced blood dyscrasia. R
Drug-related antibodies are responsible for the neutropenia in the so-called "immune" or "aminopyrine type" of agranulocytosis. R
The three types of drug-induced agranulocytosis:
Three distinct mechanistic types of drug-induced agranulocytosis have been characterized: R
- The aminopyrine type: sudden destruction of large numbers of peripheral blood neutrophils by drug-dependent antibodies elicited in sensitized individuals
- The procainamide type: a lupus-like syndrome followed by leucopenia R
- The chlorpromazine type: a latent-period reaction involving bone marrow insufficiency in patients with limited marrow proliferative potential R
Aminophenazone is the defining example and historical prototype of the first type. R
The reactive dication mechanism:
Aminophenazone is oxidized by myeloperoxidase (MPO) in activated neutrophils, using hypochlorous acid as the oxidant, to generate a highly reactive dication intermediate. R
This reactive dication acts as a hapten, binding covalently to neutrophil membrane proteins and creating a drug-protein adduct that the immune system does not recognize as self. R
The hapten-modified neutrophil surface triggers generation of drug-dependent anti-neutrophil antibodies (DDAbs). R
Drugs associated with a high incidence of idiosyncratic agranulocytosis generally share the property of being relatively easy to oxidize to reactive metabolites; aminopyrine fits this pattern alongside clozapine, amodiaquine, procainamide, dapsone, propylthiouracil, and vesnarinone. R
Antibody characteristics:
In a study of 13 patients with drug-related immune agranulocytosis (including patients taking metamizole, dimethylaminophenazone, and propyphenazone), competitive ELISA detected IgG and IgM class DDAbs and autoantibodies in the majority of cases. R
The DDAbs recognized drug metabolites rather than the native unmetabolized compound: they were reactive with ex vivo antigens from urine of individuals receiving therapeutic drug levels, but not with the native drugs alone in most cases. R
This metabolite-specificity confirms that the reactive dication formed by myeloperoxidase oxidation, not the parent aminophenazone molecule, is the proximate sensitizing hapten. R
The clinical course:
On first exposure, agranulocytosis typically develops after a latent sensitization period of weeks to months as antibodies are generated. R
In sensitized individuals with pre-formed DDAbs, re-administration leads to rapid antibody binding to the reactive dication on the neutrophil surface, complement-mediated lysis, and Fc-receptor-mediated phagocytosis in the spleen and liver. R
On rechallenge, the reaction is almost immediate; rechallenge usually results in immediate neutrophil destruction and fever, producing a shorter time-to-onset than most other idiosyncratic agranulocytoses. R
Incidence and mortality:
Cumulative data show severe neutropenia or agranulocytosis from non-chemotherapy drug exposure ranges from approximately 1.6 to 15.4 cases per million population per year. R
Dipyrone (the related compound) leads the list of drugs most often associated with neutropenia or agranulocytosis in countries where it remains in use. R
Case fatality rates from established agranulocytosis before modern intensive care and G-CSF (granulocyte colony-stimulating factor) treatment were substantial. R
Treatment with G-CSF can hasten neutrophil recovery, but drug avoidance remains the primary prevention strategy. R
Why animal models failed:
Despite strong evidence for an immune mechanism, no reliable animal model of aminophenazone-induced agranulocytosis was established after decades of attempts. R
Rabbits treated chronically with aminophenazone (200 to 900 mg/kg/day) in 1930s experiments showed initial leukocytosis but no sustained neutropenia. R
Addition of the immune stimulator poly(I:C) to high-dose aminophenazone or dipyrone in Brown Norway rats also failed to produce agranulocytosis. R
The species-specific nature of the reaction likely reflects differences in neutrophil myeloperoxidase activity, immune tolerance mechanisms, and HLA-dependent antigen presentation between humans and standard preclinical species. R
This failure represents a fundamental challenge in IDR toxicology: the most clinically important safety signals for this class of reaction cannot be reliably detected in standard preclinical testing. R
The Nitrosamine Problem
A second and independent reason for aminophenazone's US withdrawal was its ability to react with nitrite-containing foods and gastric nitrous acid to form carcinogenic N-nitrosamines. R
The chemical mechanism:
Aminophenazone contains a secondary dimethylamino group. R
Under acidic conditions (such as the stomach's low-pH environment, particularly in the presence of dietary nitrites from cured meats, preserved vegetables, and other nitrite-containing foods), this dimethylamino group reacts with nitrous acid to form dimethylnitrosamine and related N-nitrosamine compounds. R
The methylated nitrogen derivative aminopyrine was introduced in 1897 and specifically taken off the US market in the 1970s because of this nitrosamine-forming property. R
N-nitrosamines are potent hepatocarcinogens in animal models and are classified as probable human carcinogens. R
The concern was that chronic aminophenazone use in patients consuming nitrite-containing foods could generate meaningful gastric nitrosamine exposure over years of treatment. R
Regulatory action:
The FDA cited both the agranulocytosis risk and the nitrosamine formation potential when suspending aminophenazone from commercial use in 1977, with this suspension formally restated in 1999. R
The WHO Drug Information bulletin in 1977 noted that products containing aminophenazone had been formally withdrawn in many countries and marketing had been voluntarily suspended in others. R
The nitrosamine concern added a carcinogenic risk dimension on top of the already-established hematologic toxicity, making the benefit-risk calculation unfavorable given available alternatives. R
The mechanism (a secondary amine group forming N-nitrosamines under acidic conditions with gastric nitrous acid) is chemically analogous to what drove the ranitidine, valsartan, and metformin nitrosamine recalls from 2018 to 2022, making aminophenazone an early case study in the same regulatory problem. R
The Aminopyrine Breath Test: A Lasting Scientific Legacy
Despite aminophenazone's clinical withdrawal as an analgesic, its unique hepatic metabolism provided a lasting contribution to hepatology: the aminopyrine breath test (APBT), a non-invasive measure of hepatic CYP450 microsomal function. R
The principle:
When radiolabeled aminophenazone (¹⁴C-labeled or ¹³C-labeled at the N-methyl groups) is administered orally, CYP450 enzymes in the liver N-demethylate the compound, releasing labeled methyl groups that are metabolized to labeled carbon dioxide (¹⁴CO₂ or ¹³CO₂) and exhaled. R
The rate of labeled CO₂ in exhaled breath directly reflects the functional microsomal mass of the liver: specifically, the amount of active CYP enzyme capable of performing N-demethylation at that moment. R
Percent dose recovered as ¹⁴CO₂ at 2 hours correlates highly with aminopyrine metabolic clearance rate (r = 0.92), serum albumin (r = 0.75), and bromsulphalein retention (r = 0.73), establishing it as a valid hepatocellular functional measure. R
Clinical validation across liver disease conditions:
Normal breath test value: 7.0 ± 1.3% dose per 2 hours as ¹⁴CO₂. R
Reduced values occur in: R
- Portal cirrhosis: 2.6 ± 1.2%
- Fatty liver: 4.7 ± 1.1%
- Acute hepatitis: 2.6 ± 1.4%
- Hepatic malignancy: 3.5 ± 1.8%
Values return to normal when hepatitis resolves, and the breath test proved more sensitive to treatment effects than conventional tests: 2 weeks of prednisolone therapy produced measurable improvement in 9 of 10 patients with chronic active hepatitis. R
Patients taking enzyme-inducing drugs such as phenobarbitone showed above-normal values (due to CYP induction), as did some alcoholic patients without cirrhosis. R
In alcoholic hepatitis, the normal value for the breath test was 8.6 ± 1.5%, while patients with alcoholic cirrhosis averaged 5.1 ± 3.8%. R
Mortality prediction in alcoholic hepatitis:
In a prospective study of 51 hospitalized patients with alcoholic hepatitis followed for 3 weeks, only an aminopyrine breath test greater than 1% of administered dose as ¹⁴CO₂ at 2 hours correlated with 3-week survival (P = 0.0075). R
Only an increase of more than 100% in breath test value was associated with clinical improvement (P = 0.0036). R
In the subgroup with histologically confirmed alcoholic liver disease, the aminopyrine breath test correlated with histologic severity better than conventional liver function tests including bilirubin, albumin, and prothrombin time. R
Where the test fails:
The aminopyrine breath test does not reliably detect cirrhosis in cholestatic liver disease. R
In 19 cholestatic patients (primary biliary cirrhosis, sclerosing cholangitis, chronic extrahepatic bile duct obstruction), breath test results in those with cirrhosis were not significantly different from those in precirrhotic cholestatic patients (mean 11.2 ± 5.0% vs. 11.6 ± 2.8%) or healthy subjects (11.5 ± 2.9%). R
Decreased microsomal enzyme function appears to be a late feature of cholestatic liver disease, unlike hepatocellular disease where it occurs relatively early. R
The test also offers no obvious diagnostic advantage over serum albumin measurement in distinguishing hepatocellular from cholestatic disease. R
Confounders that require careful interpretation:
Results are significantly influenced by multiple factors beyond liver function per se. R
CYP2C19 poor metabolizers produce falsely low values that can mimic hepatocellular disease even in healthy individuals, and this polymorphism must be considered when interpreting breath test results in clinical practice. R
Oral contraceptive steroid use suppresses values by approximately 50% during active use (6.1 ± 2.3% vs 12.1 ± 1.6% in non-users), reversing within 7 days of stopping. R
Cigarette smoking induces CYP1A2 and raises values above non-smoker baseline. R
The combined effect of smoking and oral contraceptive steroid use results in approximately unchanged overall metabolic activity due to opposing induction and inhibition. R
Enzyme-inducing drugs raise values; enzyme inhibitors lower them. R
A study of 110 healthy subjects confirmed large inter-individual variation in ¹³C-aminopyrine breath test values in accordance with natural variability in hepatic CYP450 content, with cigarette smoking and oral contraceptive steroids both producing statistically significant shifts in opposite directions. R
Current status:
The ¹³C-aminopyrine breath test (non-radioactive stable isotope) replaced the original ¹⁴C version (radioactive), making it safer for routine clinical use. R
Both the ¹³C-aminopyrine and the ¹³C-methacetin breath tests can play a role in assessing microsomal liver function and may be useful in following progressive hepatocellular disease. R
The perfect drug probe to assess the full functional metabolic capacity of the liver has not been identified; methacetin has largely supplanted aminopyrine in clinical practice because methacetin does not carry aminophenazone's carcinogenicity concerns. R
Neither is FDA-approved as a diagnostic test; both are used primarily in research settings. R
Dipyrone (Metamizole): The Related Compound Still In Use
Dipyrone (metamizole sodium) is the sodium sulfonate salt of a methylaminoantipyrine, metabolized to 4-aminoantipyrine, the same primary active metabolite as aminophenazone. R
Dipyrone has been in clinical use since 1922. R
Dipyrone shares aminophenazone's analgesic and antipyretic mechanisms (COX inhibition and PAG-mediated descending inhibition) and shares its agranulocytosis risk through the same reactive metabolite and drug-dependent antibody pathway. R
Drug-dependent anti-neutrophil antibodies reactive to dipyrone metabolites have been documented in affected patients using competitive ELISA: in a series of 13 agranulocytosis patients, those associated with metamizole had IgG and IgM class DDAbs that were reactive to ex vivo metabolite antigens in urine from drug-treated donors, but not to the native unmetabolized drug in most cases. R
Despite this, dipyrone remains widely used in Germany, Brazil, Mexico, Spain, Israel, and numerous other countries, where clinicians argue that its agranulocytosis risk (estimated at 1 to 10 per million treatment episodes in modern pharmacovigilance studies) is acceptable given its efficacy for colicky pain, renal colic, and high-grade fever where other analgesics fail. R
Drugs most often associated with immune neutropenia or agranulocytosis include dipyrone, diclofenac, ticlopidine, calcium dobesilate, spironolactone, antithyroid drugs, and carbamazepine. R
Dipyrone leads this list in countries where it remains in wide clinical use. R
It is banned in the United States, United Kingdom, Australia, and many other countries. R
The dipyrone debate illustrates the fundamental disagreement in international drug regulation about acceptable risk-benefit trade-offs for a drug that is effective and inexpensive but carries a rare but potentially fatal idiosyncratic toxicity. R
The US and UK concluded the risk was unacceptable given available alternatives; Germany and Brazil reached the opposite conclusion. R
Dipyrone is included here because it is the most clinically relevant surviving member of the aminopyrine drug family, and because readers encountering "metamizole" in international medical literature should understand its chemical relationship to aminophenazone and the shared toxicity mechanism. R
Regulatory Status Worldwide
| Country / Region | Status |
|---|---|
| United States | FDA suspended 1977; use prohibited R |
| France | Withdrawn R |
| Japan | Withdrawn (Committee on Safety of Drugs order) R |
| India | Banned R |
| Thailand | Banned R |
| Most EU countries | Withdrawn or restricted |
| Germany, Brazil, Mexico, Spain, Israel | Dipyrone (related compound) still in use R |
| Developing world | Aminophenazone still in use in some markets R |
The FDA's suspension cited two independent grounds: (1) agranulocytosis risk with documented fatalities, and (2) in vivo nitrosamine formation potential. R
Japan's Committee on the Safety of Drugs ordered withdrawal because of these serious adverse effects. R
In countries where aminophenazone or dipyrone remain in use, leukocyte count and differential should be monitored during administration of large doses or continued use of small doses. R
Restrictions on duration of use, mandatory hematologic monitoring, and warnings against use in previously sensitized patients are standard requirements. R
Genetics
CYP2C19 (rs4244285, rs4986893, and others):
CYP2C19 is a principal enzyme in aminophenazone N-demethylation and an important genetic determinant of both drug exposure and aminopyrine breath test values. R
Poor metabolizers (two loss-of-function CYP2C19 alleles) clear aminophenazone substantially more slowly, raising drug exposure and producing breath test values that falsely mimic hepatocellular dysfunction. R
CYP2C19 poor metabolizer frequency varies considerably by population: approximately 2 to 5% of Europeans versus up to 15 to 20% in some East Asian populations, making this a clinically significant source of breath test result variability across ethnic groups. R
Ultra-rapid metabolizers (CYP2C19 gene duplication) clear aminophenazone faster, reducing therapeutic duration and producing falsely elevated breath test values that could mask modest hepatic dysfunction. R
CYP1A2 and cigarette smoking:
Cigarette smoking potently induces CYP1A2, which participates in aminophenazone N-demethylation alongside CYP2C19. R
In 110 healthy subjects phenotyped for CYP1A2 activity, the ¹³C-aminopyrine breath test was sensitive enough to detect significant CYP induction from cigarette smoking and significant CYP inhibition from oral contraceptive steroids as opposing effects. R
Smokers show higher aminopyrine breath test values than matched non-smokers, a confound requiring specific adjustment in clinical interpretation. R
HLA and agranulocytosis susceptibility:
Several drugs causing immune-mediated agranulocytosis have been associated with specific HLA class II alleles. R
Clozapine-induced agranulocytosis has been associated with HLA alleles that differ by race, confirming the role of MHC class II antigen presentation in drug-dependent immune sensitization. R
Aminophenazone-induced agranulocytosis has not been systematically studied in the modern HLA genotyping era, because the drug was withdrawn before comprehensive pharmacogenomics became feasible. R
Given the established requirement for immune sensitization via hapten-modified antigen presentation on MHC class II molecules, HLA associations almost certainly exist but remain unmapped for aminophenazone specifically. R
Myeloperoxidase (MPO) variants:
Aminophenazone is oxidized by neutrophil myeloperoxidase to the reactive dication hapten that initiates immune sensitization. R
Genetic variation in MPO expression or activity would theoretically modulate the rate of reactive hapten formation in activated neutrophils and thereby influence sensitization risk in any given individual. R
MPO promoter polymorphisms (particularly the -463G/A variant) affect MPO expression levels and have been implicated in susceptibility to other MPO-dependent drug oxidation reactions. R
Whether MPO genotype predicts aminophenazone agranulocytosis risk has not been directly studied, but represents a mechanistically plausible genetic risk modifier. R
More Research
- Aminopyrine as the IDR prototype: Aminophenazone-induced agranulocytosis remains one of the best-mechanistically-characterized examples of immune-mediated idiosyncratic drug reactions (IDRs), a class of adverse effects that remains difficult to predict, prevent, and model in preclinical settings.
The aminopyrine mechanism (reactive dication formation via myeloperoxidase, hapten binding to neutrophil membrane proteins, drug-dependent antibody generation, and rapid neutrophil destruction on rechallenge) serves as a mechanistic template for understanding similar reactions caused by clozapine, ticlopidine, dapsone, propylthiouracil, and amodiaquine. R
Attempts to develop reliable animal models of aminopyrine agranulocytosis for use in new drug screening have consistently failed, highlighting a fundamental barrier in IDR toxicology: this class of human immune reaction cannot be reproduced in standard preclinical species even after decades of effort. R
- ¹³C-aminopyrine breath test in NAFLD and NASH staging: As NAFLD and non-alcoholic steatohepatitis (NASH) emerge as major causes of cirrhosis, non-invasive tools to stage disease severity and reduce reliance on liver biopsy are increasingly needed. R
Both the ¹³C-aminopyrine and ¹³C-methacetin breath tests assess microsomal liver function and may contribute to evaluating metabolic liver disease severity. R
Whether the aminopyrine breath test adds meaningful diagnostic information beyond non-invasive liver stiffness measurements (FibroScan) and serum biomarker panels in NAFLD remains an open question.
The test's sensitivity to CYP2C19 polymorphisms, oral contraceptives, smoking, and enzyme-inducing or inhibiting drugs complicates standardization across diverse clinical populations and is a significant remaining limitation. R
- The nitrosamine template for modern pharmaceutical safety:
Aminophenazone's withdrawal on nitrosamine formation grounds in 1977 predated the 2018 to 2022 global wave of pharmaceutical nitrosamine recalls by four decades.
The mechanism (a secondary amine reacting with nitrous acid under acidic conditions to form carcinogenic N-nitrosamines) is chemically analogous to what drove the valsartan, ranitidine, and metformin recalls, and the regulatory logic applied to aminophenazone anticipated the current FDA and EMA nitrosamine guidance frameworks. R
Aminophenazone's case history is directly precedent-setting for current pharmaceutical nitrosamine risk assessment, even though it is rarely cited in that modern regulatory context. R
- Dipyrone and the global pharmacovigilance debate:
The ongoing use of dipyrone (metamizole) in approximately half the world while it remains banned in the other half represents one of the longest-running unresolved disagreements in international drug regulation.
Modern pharmacovigilance studies from countries with dipyrone registries in Germany, Spain, and Brazil have produced agranulocytosis incidence estimates ranging from approximately 1 to 15 per million treatment episodes, a range wide enough to sustain opposing regulatory conclusions. R
Whether the risk-benefit calculation should favor restriction or availability depends substantially on the availability and safety profile of alternatives for the specific indications where dipyrone has been preferred (severe colicky pain, renal colic, high-grade refractory fever) and on local regulatory philosophy about acceptable rare but serious harm.
This debate is unresolved and ongoing. R
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Quercetin
500mg 2x/day
SPM Active (Pro-resolving Mediators)
2 softgels/day
Curcumin (Liposomal)
500mg 2x/day