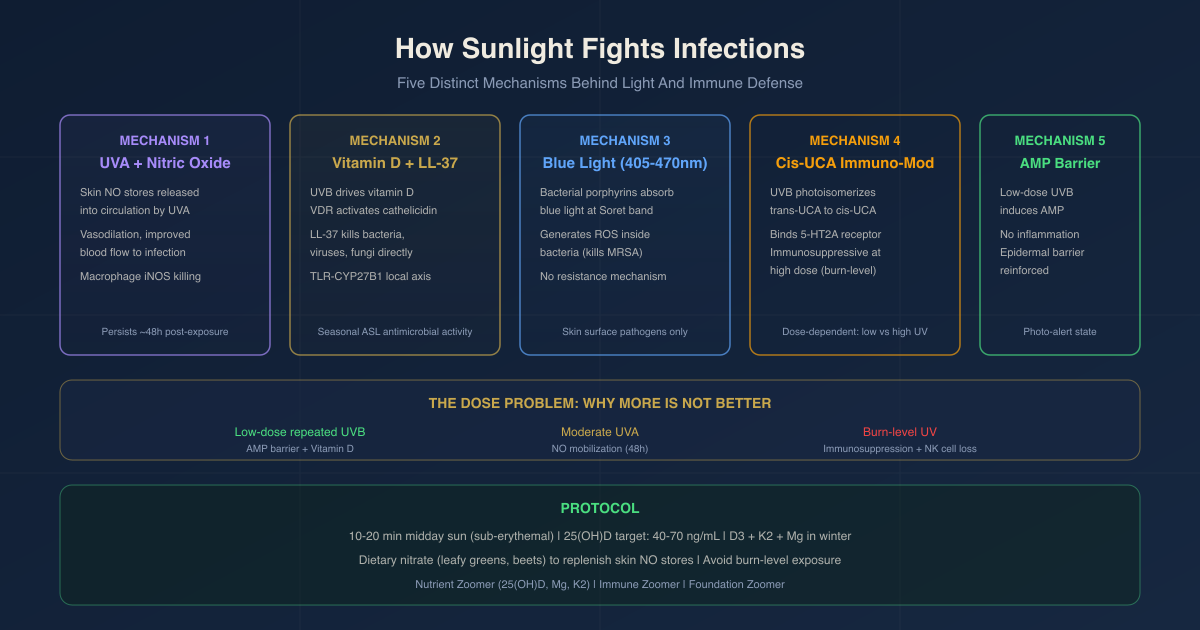
How Sunlight Fights Infections: The Real Mechanisms Behind Light And Immune Defense
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Sunlight has measurable antimicrobial and immune-modulating effects, but the mechanisms are more specific and interesting than the popular framing of "oxidizing the blood."
In this post, we will discuss the five distinct biological pathways through which sunlight exposure affects infection resistance: nitric oxide mobilization from skin stores into the bloodstream, vitamin D-driven production of antimicrobial peptides, direct antimicrobial effects of blue and near-visible light on pathogens, immunomodulation through the cis-urocanic acid pathway, and the reinforcement of the epidermal antimicrobial barrier by low-dose UVB.
The "Blood Oxidation" Claim: What The Evidence Actually Shows
The idea that sunlight "oxidizes the blood" or "purifies" blood through oxidation is not supported by the peer-reviewed literature as a discrete mechanism.
Sunlight penetrates the skin only superficially.
ultraviolet B (UVB) (290 to 315 nm) reaches only the epidermis. R
ultraviolet A (UVA) (315 to 400 nm) penetrates slightly deeper into the dermis, but does not meaningfully reach circulating blood in subcutaneous vessels. R
Visible and near-infrared light penetrates further, but not in concentrations that would produce systemic oxidative effects in the blood stream under normal sun exposure.
What sunlight does do at the skin surface is release biologically active molecules that then enter the circulation and have systemic effects.
These effects are real, well-documented, and mechanistically important, but they are not "blood oxidation."
The most significant of them is nitric oxide (NO) mobilization from skin stores into the bloodstream via UVA exposure.
Separately, sunlight drives vitamin D synthesis, which in turn regulates the production of antimicrobial peptides that kill bacteria and viruses inside immune cells.
And certain wavelengths of visible light (blue, 405 to 470 nm) directly kill bacteria at the skin surface through a photochemical mechanism.
These are the actual mechanisms worth understanding.
Mechanism 1: UVA Mobilizes Nitric Oxide From Skin Into The Circulation
The skin is the largest nitric oxide reservoir in the human body.
Nitrate levels in human skin are two to three times higher than in the circulation. R
The skin stores nitric oxide in three photolabile (light-sensitive) forms: nitrite (NO2-), nitrate (NO3-), and S-nitrosothiols (RSNOs), primarily S-nitrosoalbumin and S-nitrosoglutathione. R
When UVA radiation strikes the skin, it photolytically cleaves these stored forms, releasing free nitric oxide gas. R
That nitric oxide then diffuses from skin tissue into the dermal vasculature and enters systemic circulation as nitrite and S-nitrosothiols.
The Liu et al. 2014 clinical trial (Feelisch/Weller group, University of Edinburgh and Southampton) is the key human study here.
In 24 healthy volunteers, irradiation of the skin with two standard erythemal doses of UVA lowered blood pressure by at least 5 mmHg, increased blood flow, and produced measurable rises in circulating nitrite and S-nitrosothiol concentrations. R
The UVA-induced forearm blood flow increase occurred independently of NO synthase (NOS) activity, confirming the effect came from pre-formed skin NO stores, not from enzymatic NO production. R
Dietary nitrate manipulation did not alter the UV-induced hemodynamic changes, ruling out dietary nitrate in the skin stores as the source. R
An earlier study (Oplander et al., Circulation Research, 2009) confirmed that whole-body UVA irradiation released isotopically labeled 15N-nitrite from skin into the plasma of volunteers, and UVA enhanced dermal S-nitrosothiols 2.3-fold and S-nitrosoalbumin 2.9-fold during the exposure. R
Why this matters for infection resistance:
Nitric oxide is a primary innate immune effector.
iNOS (inducible nitric oxide synthase), expressed in activated macrophages, generates NO from L-arginine and uses it to kill intracellular microbial pathogens inside the phagosome via protein and DNA disruption. R
NO diffuses across bacterial cell membranes and exerts both nitrosative and oxidative damage on invading pathogens. R
NO from iNOS was the identified downstream killing mechanism in early models of macrophage-mediated control of Leishmania major and other intracellular pathogens. R
The antibiofilm properties of NO are also well documented, as NO can penetrate biofilm matrices and disperse biofilm-protected bacteria. R
Circulating NO released from skin by UVA irradiation enters this system by increasing systemic NO bioavailability, which feeds into macrophage-mediated killing, vasodilation (improving blood flow to infected tissues), and potentially antibiofilm activity at sites of infection.
NO persistence after UVA: A 2022 study demonstrated that NO release from keratinocytes, fibroblasts, and endothelial cells persists well beyond the period of light exposure, peaking approximately 48 hours after a moderate UVA dose. R
This is relevant clinically: the immune-relevant NO elevation from UVA skin exposure does not terminate when the sun goes down.
Mechanism 2: Vitamin D Drives Antimicrobial Peptide Production
This is the most well-characterized pathway linking sunlight to infection resistance, and it operates through the vitamin D endocrine system rather than through direct sunlight effects on blood or immune cells.
UVB converts 7-dehydrocholesterol in the epidermis to cholecalciferol, which undergoes hepatic 25-hydroxylation and renal 1-alpha-hydroxylation to produce the active hormone calcitriol (1,25(OH)2D3). R
Calcitriol binds the VDR (vitamin D receptor), which is expressed in virtually all nucleated cells, and induces transcription of genes with vitamin D response elements (VDREs) in their promoters.
Two antimicrobial peptide genes regulated by VDR are critical:
Cathelicidin (CAMP gene, active peptide: LL-37) and beta-defensin 2 (HBD2/DEFB4). R
LL-37 is a cationic amphipathic peptide that disrupts microbial membranes, activates other antimicrobial pathways inside infected cells, induces chemotaxis, and directly kills a broad range of bacteria, viruses, and fungi. R
The landmark TLR mechanism: when innate immune cells encounter pathogens, Toll-like receptor (TLR) signaling upregulates both CYP27B1 (the renal/macrophage 1-alpha-hydroxylase that converts 25(OH)D to calcitriol) and the VDR simultaneously. R
This creates a local calcitriol-VDR-cathelicidin axis inside the macrophage itself, independent of circulating calcitriol levels.
The pathway was demonstrated in Mycobacterium tuberculosis infection: TLR activation by bacterial ligands triggered CYP27B1 upregulation, local calcitriol production, and cathelicidin expression, with LL-37 then binding directly to intracellular M. tuberculosis and contributing to its killing. R
White-skinned donors had enough circulating 25(OH)D to sustain this pathway when their serum was used to culture immune cells, while serum from African American donors (lower 25(OH)D) supported significantly lower cathelicidin output. R
The vitamin D-tuberculosis (TB) connection is one of the most robust sunlight-infection links in human data.
Low 25(OH)D is a consistent risk factor for active tuberculosis across multiple systematic reviews and meta-analyses. R
Active pulmonary TB is associated with hypovitaminosis D compared with non-TB controls, and vitamin D status has a documented protective role against tuberculosis disease. R
LL-37 expression is induced in human alveolar macrophages, monocyte-derived macrophages, neutrophils, and epithelial cells by M. tuberculosis infection, and the induction is amplified by TLR-2, TLR-4, and TLR-9 stimulation. R
Seasonal antimicrobial activity in airway surface liquid:
A trial using vitamin D supplementation (1000 IU/day for 90 days) enhanced antimicrobial activity in lung airway surface liquid (ASL). R
ASL antimicrobial activity was found to be more robust in summer and fall than in winter and spring, consistent with seasonal fluctuations in circulating 25(OH)D. R
Blocking LL-37 with a specific antibody eliminated the antimicrobial activity in ASL, and the seasonal variation in activity was eliminated by vitamin D supplementation, confirming that 25(OH)D is the driver of the seasonal antimicrobial capacity of the lung. R
This is a direct mechanistic link between sunlight, circulating 25(OH)D, cathelicidin expression, and respiratory infection resistance in humans.
Mechanism 3: Blue Light Kills Pathogens Directly At The Skin Surface
The visible blue and violet portion of the solar spectrum (approximately 405 to 470 nm) has intrinsic antimicrobial properties that are independent of exogenous photosensitizers.
The mechanism: many pathogenic bacteria accumulate intracellular iron-free porphyrins and flavins that absorb maximally at 405 nm and 470 nm respectively. R
Blue light photo-excites these endogenous photosensitizers, which then transfer energy to oxygen to generate reactive oxygen species (ROS) that damage bacterial lipids, proteins, DNA, RNA, and polysaccharides. R
This mechanism kills bacteria regardless of antibiotic resistance profiles because it attacks fundamental cellular structures rather than single enzyme targets. R
Pathogens killed by antimicrobial blue light include:
Gram-positive bacteria (generally more sensitive due to a porous outer wall): R
- MRSA (methicillin-resistant Staphylococcus aureus): colony-forming unit (CFU) reductions of 72 to 81% at 28.5 J/cm2 at 412 to 450 nm R
- Streptococcus species
- Enterococcus species
Gram-negative bacteria (less sensitive due to compact outer membrane barrier): R
- Pseudomonas aeruginosa
- Escherichia coli
- Helicobacter pylori (blue light clinical trials for H. pylori stomach infections have shown promising results) R
Fungal pathogens:
Propionibacterium acnes (now renamed Cutibacterium acnes): blue light therapy at 415 nm is a clinically accepted treatment for P. acnes-driven acne, validated in multiple trials. R
The important caveat: these antimicrobial blue light doses are studied in clinical and laboratory settings using controlled light sources.
Ambient sunlight at the skin surface contains the right wavelengths but at variable intensities depending on time of day, latitude, cloud cover, and skin angle.
The direct pathogen-killing effect of solar blue light is most relevant at the skin surface, in wounds, and in mucous membranes exposed to sunlight, not systemically.
There is no meaningful penetration of blue light into deep tissues or blood.
Mechanism 4: Cis-Urocanic Acid And Immune Modulation
Urocanic acid (UCA) is a histidine metabolite present at approximately 0.7% of the dry weight of the stratum corneum (outermost skin layer). R
In its resting state it exists as trans-UCA.
UVB irradiation photoisomerizes trans-UCA to cis-UCA in a dose-dependent fashion until photostationary equilibrium with roughly equal quantities of both isomers is reached. R
Cis-UCA is a systemic immunomodulator.
It has been identified as a ligand for the 5-HT2A (serotonin) receptor, with a Kd of approximately 4.6 nM. R
Platelet-activating factor (PAF) and serotonin receptor antagonists both block cis-UCA-induced immune suppression. R
The downstream cascade involves dermal mast cell degranulation, histamine release, and prostaglandin E2 (PGE2) production by keratinocytes, which together drive systemic immunomodulation. R R
This pathway is primarily immunosuppressive, not immunostimulatory.
It reduces contact hypersensitivity responses, suppresses Langerhans cell antigen presentation, and impairs specific immune responses to pathogens in animal models including Mycobacterium and Listeria monocytogenes and Trichinella spiralis. R R
Why does this matter in the context of infection resistance?
The cis-UCA pathway represents a genuine immunosuppressive effect of sunlight, one that is relevant in two scenarios:
1. For autoimmunity and inflammatory conditions: the sunlight-driven immunosuppression through cis-UCA may explain part of the clinical benefit of phototherapy in psoriasis, eczema, and autoimmune conditions where reducing immune overactivation is therapeutic.
2. For infectious disease context: cis-UCA-mediated immunosuppression is a trade-off.
Moderate, low-dose sunlight exposure appears to reinforce barrier antimicrobial defenses (mechanism 5 below) without generating the level of cis-UCA-driven systemic immunosuppression that high-dose UV exposure produces. R
High-dose UV, the kind that causes sunburn, generates large quantities of cis-UCA and drives significant suppression of cell-mediated immunity. R
The dose-response relationship for cis-UCA-induced immunosuppression means that repeated low-dose sunlight exposure produces a very different immune environment than a single burn-level exposure. R
Mechanism 5: Low-Dose UVB Reinforces The Epidermal Antimicrobial Barrier
A 2015 study directly compared the immune effects of two UV exposure patterns in mice: a single high UV dose (2 minimal erythemal doses (MED), burn-level) versus repetitive very low doses (one-tenth of MED, four consecutive days). R
The results were sharply divergent.
Single high dose: produced a deep inflammatory state, extensive pro-inflammatory cytokine and chemokine production, and recruitment of neutrophils and macrophages to the irradiated area. R
Repetitive low dose: produced no inflammatory response, no histological alteration of epidermal cells, but drove strong induction of antimicrobial peptide (AMP) transcription, increased epidermal thickness, and increased lymphatic circulation. R
This is a "photo-induced alert state," in which the skin reinforces its defensive barrier without generating inflammation.
The UVB-induced upregulation of AMPs at the skin surface is a direct protective mechanism against skin and wound infections.
UVB upregulates AMP gene expression in human keratinocytes both in vitro and in vivo, confirmed by multiple studies. R
The barrier-reinforcing effect of low-dose UV explains why regular moderate sun exposure (as opposed to periodic intense burns) has historically been associated with more robust skin defenses, and why heliotherapy (controlled sunlight exposure) was used as a treatment for skin infections including tuberculosis of the skin (lupus vulgaris) before antibiotics. R
The Dose Problem: Why More Is Not Better
The dose-response relationship for sunlight and immune function is not linear.
Low-dose, repeated UVB:
Reinforces epidermal barrier antimicrobial peptide expression, drives incremental vitamin D synthesis without generating large cis-UCA pools, and does not significantly suppress systemic cell-mediated immunity. R
Moderate UVA:
Mobilizes NO from skin stores into circulation (the Liu et al. cardiovascular mechanism), persisting for up to 48 hours post-exposure. R
High-dose UV (burn level):
Drives cis-UCA-mediated systemic immunosuppression, reduces natural killer (NK) cell cytotoxicity significantly, and can halve the phagocytic and chemotactic activity of neutrophils following a single whole-body exposure. R
NK cell activity in humans was reduced in all subjects after 10 days of BB-UVB at psoriasis treatment doses, taking several weeks to recover. R
A single whole-body UVB exposure at one minimal perceptible erythemal dose reduced adhesion and phagocytic abilities of phagocytic leukocytes by 50% via downregulation of complement receptors and IgG Fc receptors including CD16 (FcγRIII). R
The immunosuppressive properties of high-dose UV are the mechanistic basis of UV phototherapy for autoimmune skin disease, and the same properties explain why high UV exposure can transiently impair resistance to infection.
This means the protocol for using sunlight as an infection-resistance tool is about regularity and moderate dose, not intensity.
Seasonal Infections And Latitude: The Real-World Signal
The epidemiological data is consistent with the mechanisms above.
Cardiovascular disease incidence correlates with latitude and rises in winter, and the Liu/Weller group proposed UV-induced NO mobilization as a partial explanation. R
Respiratory infections peak in winter, which is also when 25(OH)D levels are lowest and ASL antimicrobial activity is most impaired. R
Low 25(OH)D is a consistent predictor of increased susceptibility to tuberculosis, respiratory tract infections, and other infectious diseases across large epidemiological studies.
The seasonal antimicrobial activity of airway surface liquid tracked with vitamin D levels, not with other seasonal environmental factors, providing a direct mechanistic line between reduced winter sunlight and reduced respiratory antimicrobial defense. R
There is a MAYBE here on the relative contributions of vitamin D versus other sunlight mechanisms (NO, UVA immunomodulation, AMP induction) to seasonal infection patterns.
Most of the human trial data supports vitamin D and cathelicidin as the primary pathway for the seasonal respiratory infection signal, with NO and other mechanisms having cardiovascular and skin-local relevance that is harder to quantify epidemiologically.
How To Apply This: Protocol
1. Regular Moderate Sun Exposure Without Burning
The goal is to accumulate repeated low-dose UVB for AMP barrier reinforcement and vitamin D synthesis, plus moderate UVA for NO mobilization, without reaching burn-level UV doses that drive cis-UCA immunosuppression.
10 to 20 minutes of midday sun exposure (when UVB is at adequate angle, roughly late spring through early fall at latitudes below 35 degrees) on a significant skin surface area without sunscreen is the practical target.
This dose is sub-erythemal for most adults and produces the "photo-alert" state without immunosuppressive burn-level cis-UCA generation.
For those who cannot achieve adequate sun exposure (high latitude, winter, indoor work, dark skin requiring more exposure time), vitamin D3 supplementation is the non-negotiable fallback for the cathelicidin/LL-37 mechanism specifically.
2. Optimize 25(OH)D To Maintain Cathelicidin Capacity
The vitamin D to cathelicidin pathway requires circulating 25(OH)D to be available for macrophage CYP27B1-mediated local activation when TLR stimulation occurs during infection.
A target 25(OH)D of 40 to 70 ng/mL maintains this reserve throughout the year.
Most people cannot maintain this through winter sunlight alone at latitudes above 35 degrees and require supplementation.
Add Vitamin K2 MK-7 200 mcg and Magnesium Glycinate alongside D3 for full cofactor support as outlined in the vitamin D conversion post.
3. Support NO Substrate Availability
The UVA-released NO from skin stores comes from the skin's nitrate/nitrite/S-nitrosothiol pool.
Dietary nitrate (from leafy greens, beets, arugula, and spinach) replenishes the nitrate stores in skin and supports the skin NO reservoir that UVA then mobilizes. R
4. Avoid Burn-Level Exposure, Especially If Immunocompromised
If you are dealing with active infection, immune compromise, or ongoing chronic illness, burn-level UV exposure (erythema) drives the cis-UCA and NK cell suppression pathways.
Moderate, sub-erythemal exposure provides the beneficial mechanisms without the immunosuppressive dose.
Testing
Blood Markers
The most actionable marker is serum 25(OH)D, reflecting the vitamin D store available for macrophage TLR-driven cathelicidin production.
Testing in late winter captures the annual nadir and reveals whether your sunlight and supplement strategy is maintaining adequate levels year-round.
Functional immune markers relevant to this post include neutrophil phagocytic activity and NK cell cytotoxicity, but these are research-grade assays not routinely available in functional lab panels.
Lab Panels
I use the Nutrient Zoomer (Vibrant Wellness) to assess 25(OH)D alongside magnesium, vitamin K2, and other micronutrients that influence the vitamin D to cathelicidin pathway.
I use the Immune Zoomer (Vibrant Wellness) to assess systemic immune function including complement markers, mast cell markers, and autoantibody patterns that are relevant when interpreting whether the immunomodulatory effects of sunlight are working for or against a patient's specific immune phenotype.
For people with recurrent respiratory or skin infections, the Foundation Zoomer provides baseline CBC, white blood cell differential, and inflammatory markers.
Mechanisms Of Action
Simple:
- UVA from sunlight breaks down nitric oxide stored in the skin as nitrite and S-nitrosothiols, releasing NO into the bloodstream where it dilates vessels, improves circulation to infected tissues, and contributes to macrophage pathogen-killing capacity.
- UVB drives vitamin D synthesis; active vitamin D then turns on genes for antimicrobial peptides (cathelicidin LL-37, beta-defensin 2) in macrophages and epithelial cells that directly kill bacteria, viruses, and fungi.
- Blue light in the 405 to 470 nm range kills bacteria at the skin surface by photoexciting their own porphyrin and flavin pigments into producing toxic reactive oxygen species.
- UVB converts trans-urocanic acid in the outer skin to cis-urocanic acid, which is immunosuppressive at high doses (burn-level UV) and immunomodulatory at low doses.
- Repeated low-dose UVB (sub-erythemal) induces antimicrobial peptide expression in keratinocytes and reinforces the skin barrier against pathogen entry.
Advanced:
- UVA-NO photochemistry: UVA at 320 nm is the most effective wavelength for cleaving NO from skin NO2- and NO3-. R Photolysis of nitrite produces NO and nitrogen dioxide. S-nitrosothiols cleave at the S-N bond under UVA to release NO. R Released NO then enters the dermal vasculature, where it signals through soluble guanylyl cyclase (sGC) in vascular smooth muscle cells to produce cyclic guanosine monophosphate (cGMP)-mediated vasodilation. R NOS-inhibitor experiments confirmed the released NO is from pre-formed stores, not from NOS-catalyzed L-arginine oxidation. R In the circulation, NO is carried as nitrite and S-nitrosothiols, providing sustained bioavailable NO for macrophage iNOS-mediated killing. R Macrophages use the high concentration flux of iNOS-derived NO within the phagosome to damage invading bacteria via protein nitrosylation, iron-sulfur cluster disruption, and DNA strand breaks. R
- VDR-cathelicidin axis: Calcitriol (1,25(OH)2D3) binds VDR, which heterodimerizes with RXR and binds vitamin D response elements (VDREs) in the promoters of the CAMP gene (encoding hCAP-18/LL-37) and DEFB4 (encoding HBD2). R In macrophages, TLR activation by pathogen ligands simultaneously upregulates CYP27B1 and VDR expression, creating a local autocrine loop that does not depend on circulating calcitriol. R This local 25(OH)D-to-calcitriol conversion within the macrophage requires adequate circulating 25(OH)D as substrate; when 25(OH)D is low, the macrophage cannot sustain LL-37 production at the moment of TLR activation. R LL-37 is a 37-amino acid cationic amphipathic alpha-helical peptide that inserts into and disrupts microbial lipid bilayers, forming pores that depolarize and kill bacteria and enveloped viruses. R
- Blue light porphyrin ROS mechanism: Endogenous bacterial porphyrins absorb maximally at 405 nm (the Soret band). R Photo-excited porphyrins undergo Type I and Type II photochemical reactions: Type I transfers energy via electron transfer producing superoxide radical (O2-), hydrogen peroxide (H2O2), and hydroxyl radical (OH•); Type II transfers energy directly to triplet oxygen to generate singlet oxygen (1O2). R These ROS damage bacterial cell membranes, oxidize proteins in the cell wall, and fragment bacterial DNA and RNA. R Mammalian cells are less susceptible because they contain more efficient antioxidant defense systems and are less dependent on porphyrins as metabolic intermediates than bacteria. R
- Cis-UCA serotonin receptor mechanism: trans-UCA in the stratum corneum absorbs UVB with high efficiency due to structural similarity to UV-absorbing amino acids. R Photoisomerization to cis-UCA produces a molecule structurally similar to serotonin (5-HT). R Cis-UCA binds the 5-HT2A receptor with a Kd of approximately 4.6 nM, activating intracellular calcium flux. R The cis-UCA/5-HT2A signal activates dermal mast cells, which degranulate and release histamine. R Histamine then stimulates keratinocyte PGE2 production through H1/H2 receptor signaling, and PGE2 drives downstream T cell suppression and impaired antigen presentation. R Blocking either histamine receptors or PGE2 synthesis (indomethacin) each halved UVB-induced systemic contact hypersensitivity suppression, and the effects were not additive, confirming they act in the same pathway. R
- Low-dose UVB barrier reinforcement: Very low UVB doses (one-tenth of MED), when repeated over consecutive days, induce AMP transcription without activating the inflammation or cis-UCA immunosuppressive cascade that higher doses trigger. R The AMPs upregulated include beta-defensins and cathelicidin in keratinocytes, and the effect is associated with mild thickening of the epidermis (increased stratum spinosum depth) without metabolic dysfunction or histological damage. R Lymphatic circulation in the irradiated skin is increased, which may improve immune surveillance and pathogen clearance from the skin compartment. R
More Research
- Cis-UCA is more similar in structure to serotonin (5-HT) than to its trans-isomer counterpart, which explains why it functions as a serotonin receptor agonist despite being a histidine catabolite unrelated to tryptophan metabolism. R This cross-reactivity represents a rare example of a UV-photoproduct in skin hijacking a major neurotransmitter receptor system.
- Human skin nitrate levels are two to three times higher than circulating blood nitrate, representing an evolved photolabile NO reservoir that is released on UV exposure. R The skin's NO storage capacity appears to be one of its primary metabolic functions beyond barrier and immune defense.
- Bacteriophage (prophage) genes within lysogenic bacteria can be activated by blue light, triggering bacterial lysis from within. R This is a secondary antimicrobial mechanism of blue light beyond the porphyrin ROS pathway.
- Preexposure to UVA prior to a UVB immunosuppressive protocol can partially counteract the UVB-induced suppression of delayed-type hypersensitivity responses to Listeria monocytogenes infection in mice, suggesting that the balance between UVA and UVB wavelengths in natural sunlight modulates the net immunological outcome. R Full-spectrum sunlight is not equivalent to isolated UVB in its immune effects.
- iNOS-derived NO in macrophages is not the only innate NO source relevant to infection. Constitutive endothelial NOS (eNOS) and neuronal NOS (nNOS) also produce NO at lower levels during infection and autoimmunity, and their contributions to pathogen killing and immune cell signaling are increasingly recognized as distinct from iNOS. R
- The antimicrobial blue light effect extends to MRSA and multi-drug resistant Acinetobacter baumannii, pathogens for which antibiotic options are increasingly limited, and there are no known resistance mechanisms to light-induced ROS production from endogenous porphyrins because resistance would require elimination of porphyrins that are essential for bacterial energy metabolism. R
- Mycobacterium leprae (leprosy) has evolved a specific immune evasion strategy that involves microRNA regulation of CYP27B1 and IL-1beta expression in macrophages, reducing local calcitriol production and thereby blunting the TLR-vitamin D-cathelicidin axis that M. tuberculosis cannot suppress in the same way. R This represents an evolved pathogen countermeasure to the vitamin D-cathelicidin arm of innate immunity.
For biomarker testing I use the Nutrient Zoomer to assess 25(OH)D and the Immune Zoomer to assess functional immune markers relevant to sunlight-mediated immune modulation.
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Quercetin
500mg 2x/day
Vitamin D3 + K2
5000 IU + 200mcg/day
Magnesium Glycinate
400mg at bedtime