Fecal Microbiota Transplantation: What It Is, How It Works, And What The Evidence Actually Shows
By Jacob Gordon, INHC, FMT-CThis article contains affiliate links. As an Amazon Associate, MyBioHack earns from qualifying purchases at no extra cost to you. We only link products we research and stand behind.
Fecal microbiota transplantation (FMT) is the transfer of processed stool from a healthy screened donor into the gastrointestinal tract of a recipient, with the goal of restoring a depleted or dysbiotic microbiome.
In this post, we will discuss what FMT is, why it works mechanistically, where the evidence is strong, where it is weak, what the delivery options and regulatory landscape look like, what the real risks are, and what is coming next.
What FMT Is And Where It Came From
The concept of transferring intestinal contents from a healthy individual to a sick one is not new.
The earliest documented use is from 4th century China, where a physician named Ge Hong described administering human fecal suspension orally to patients with food poisoning and severe diarrhea.
In 1958, Ben Eiseman at the University of Colorado published the first modern case series describing four patients with pseudomembranous colitis treated with fecal enemas, all of whom recovered. R
For the next five decades the procedure remained a curiosity.
Then in 2013, a landmark Dutch randomized controlled trial published in NEJM showed that FMT via duodenal infusion was dramatically more effective than vancomycin for recurrent Clostridioides difficile (C. difficile) infection: 81% resolution with FMT versus 31% with vancomycin alone. R
That trial transformed FMT from a medical curiosity into an evidence-based therapy.
Since then, multiple professional societies including the American Gastroenterological Association (AGA), the American College of Gastroenterology (ACG), and the Infectious Diseases Society of America (IDSA) have issued guidelines supporting FMT use in recurrent C. difficile.
The FDA approved the first standardized FMT-derived products in 2022 and 2023, moving the field from artisanal stool transfers toward regulated biologic drugs.
Why The Gut Microbiome Breaks Down In The First Place
A healthy gut microbiome contains approximately 10^13 microorganisms across an estimated 1,000 species, spanning bacteria, archaea, fungi, viruses (especially bacteriophages), and eukaryotic parasites.
Healthy microbial diversity performs functions the host cannot perform itself:
- Converting primary bile acids to secondary bile acids via bile salt hydrolase (BSH) and 7alpha-dehydroxylase activity (critical for pathogen resistance)
- Fermenting dietary fiber to short chain fatty acids (SCFAs) including butyrate, propionate, and acetate
- Competing for nutrients and physical attachment sites, preventing pathogen colonization
- Producing bacteriocins and other antimicrobials that suppress pathogens
- Educating and modulating the mucosal immune system
- Maintaining epithelial barrier integrity via butyrate-dependent signaling
Dysbiosis is loss of this functional ecological balance.
It occurs primarily through:
- Broad-spectrum antibiotic use (the most common and well-documented cause)
- Repeated hospitalization
- Proton pump inhibitor (PPI) use
- Enteral or parenteral nutrition
- Chemotherapy
- Bowel prep for colonoscopy
- Inflammatory bowel disease
- Aging and loss of microbial diversity over decades
The more completely a microbiome is wiped out by antibiotics, the longer recovery takes and the more vulnerable the gut becomes to colonization by opportunistic pathogens like C. difficile.
How C. difficile Infection Becomes Recurrent And Why Antibiotics Fail
Clostridioides difficile is a Gram-positive, anaerobic, spore-forming bacterium.
Spores are the key to its persistence: they are resistant to alcohol, heat, desiccation, and most surface disinfectants (requiring bleach or sporicidal agents), and can survive on hospital surfaces for months.
Normal pathogenesis:
Spores are ingested, survive gastric acid, and germinate in the colon.
In a healthy microbiome, colonization resistance from commensal bacteria prevents C. difficile from proliferating.
After antibiotic disruption of the microbiome, this colonization resistance fails.
C. difficile proliferates, produces Toxin A (TcdA) and Toxin B (TcdB), which inactivate Rho family GTPases in colonocytes, causing cytoskeletal collapse, cell death, and the characteristic pseudomembranous colitis.
Severity ranges from mild diarrhea to fulminant colitis with toxic megacolon and death.
CDI causes more than 500,000 infections and approximately 29,000 deaths per year in the United States. R
Why recurrence happens:
After a first episode of CDI treated with vancomycin or fidaxomicin, approximately 20-35% of patients experience recurrence.
After the first recurrence, the risk of a second recurrence rises to approximately 40-65%.
The mechanism is a vicious cycle: antibiotics used to treat CDI further deplete the already-depleted microbiome, perpetuating the conditions that allowed C. difficile to thrive in the first place.
Each course of antibiotics digs the ecological hole deeper.
The surviving spores germinate as soon as antibiotic pressure lifts.
Without a restored microbiome to provide colonization resistance, the cycle repeats indefinitely.
Vancomycin targets vegetative C. difficile bacteria but does not kill spores and does not restore the microbiome.
Fidaxomicin is somewhat better: its narrow spectrum spares more commensal bacteria, but it still does not restore the ecosystem that would prevent regrowth from spores. R
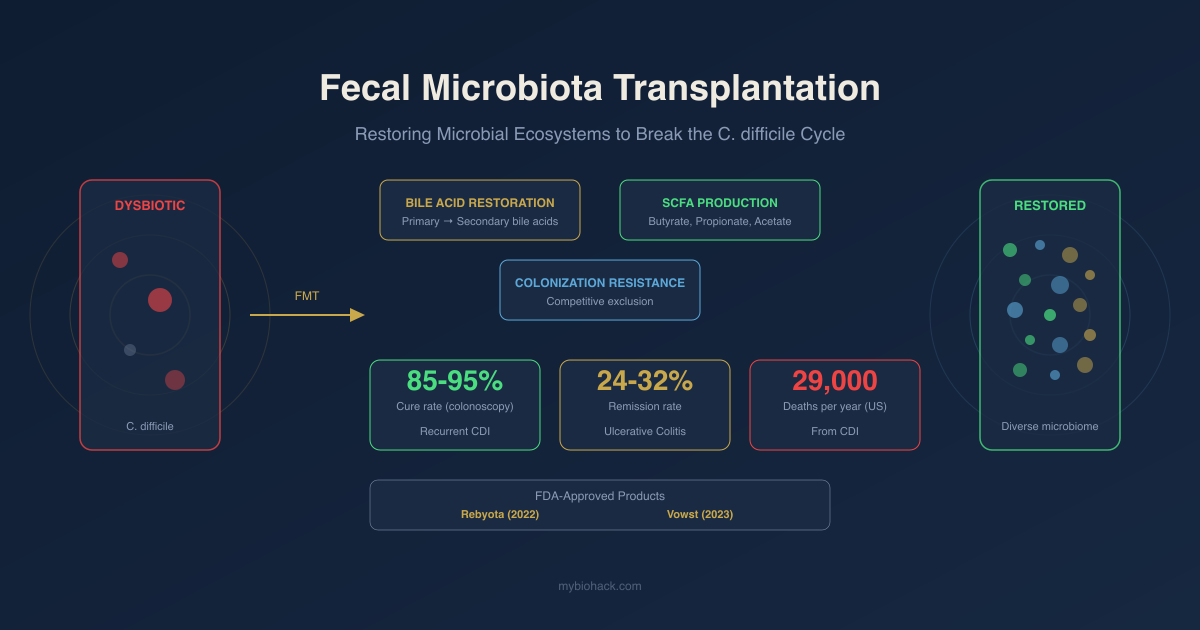
The Mechanisms Of FMT: How It Actually Works
FMT works by transferring not just bacteria but an entire functional ecosystem, including metabolites, bacteriophages, fungi, and the biochemical functions encoded by that ecosystem's collective genome.
The three primary mechanisms are:
1. Bile acid metabolism restoration (most critical for C. difficile)
2. Short chain fatty acid production restoration
3. Direct colonization resistance via competitive exclusion and nutrient competition
A fourth mechanism, immune modulation, appears increasingly important for non-CDI applications.
The fact that FMT achieves 80-90% success rates for recurrent CDI while transferring thousands of microbial species simultaneously has made it difficult to identify the single critical components.
This is why the field is still working to develop defined consortia that can replicate FMT's effect with known and controlled inputs.
Bile Acid Biology: The Central Mechanism For C. difficile
Bile acid metabolism is the most mechanistically understood pathway by which FMT prevents C. difficile recurrence. R
Primary bile acids are synthesized in the liver from cholesterol (cholic acid and chenodeoxycholic acid), conjugated with taurine or glycine, and secreted into the bile.
In the gut, gut bacteria perform two key transformations:
Deconjugation: Bile salt hydrolases (BSHs), expressed by a wide range of commensal bacteria including Lachnospiraceae and Ruminococcaceae, cleave the taurine or glycine conjugate from primary bile acids.
7alpha-dehydroxylation: Specific bacteria encoding the bile acid inducible (bai) operon (most importantly Clostridium scindens) convert deconjugated primary bile acids to secondary bile acids, primarily deoxycholic acid (DCA) and lithocholic acid (LCA).
Why this matters for C. difficile:
Conjugated primary bile acids, particularly taurocholate (TCA), are required for C. difficile spore germination.
This is mechanistically logical: C. difficile spores use primary bile acids as a signal that they have arrived in the intestinal environment, triggering germination.
Secondary bile acids (DCA, LCA, and their epimers like isoDCA and isoLCA) potently inhibit both C. difficile spore germination and vegetative growth.
In a dysbiotic gut after antibiotics, BSH-producing and bai-operon-containing bacteria are depleted.
Primary bile acids accumulate.
C. difficile spores encounter abundant germination signals and no inhibitory secondary bile acids.
Germination and regrowth follow.
After FMT, BSH-producing Lachnospiraceae return.
Secondary bile acid production is restored within days.
The germination signal environment shifts from pro-germination to anti-germination.
C. difficile spores that survive cannot establish vegetative growth. R
Metagenomic studies of FMT recipients show a clear shift from conjugated primary bile acid-dominant profiles pre-FMT to secondary bile acid-dominant profiles post-FMT, tracking directly with clinical cure.
Microbially conjugated bile acids (MCBAs), also called bacterial bile acid amidates, have recently been identified as an additional layer of bile acid regulation post-FMT, with potential inhibitory effects on C. difficile that are still being characterized.
Short Chain Fatty Acids And Colonization Resistance
Short chain fatty acids (SCFAs), produced by bacterial fermentation of dietary fiber, are substantially depleted in patients with CDI and in antibiotic-treated individuals. R
The three primary SCFAs are butyrate, propionate, and acetate.
After FMT for recurrent CDI, sustained increases in all three SCFAs are observed in stool and correlate with clinical resolution.
How SCFAs suppress C. difficile and restore the intestinal environment:
- Butyrate is the primary energy source for colonocytes, supporting epithelial barrier integrity and tight junction protein expression
- Butyrate promotes regulatory T cell (Treg) differentiation through histone deacetylase inhibition, dampening inflammatory responses
- Acidification of luminal pH from SCFA production creates an environment hostile to many pathogens including C. difficile
- SCFAs suppress the growth of multiple opportunistic pathogens through direct antimicrobial mechanisms
Butyrate also increases C. difficile toxin production and sporulation in certain conditions, a counterintuitive finding that highlights the complexity of these ecological interactions and the importance of the full microbial context rather than any single metabolite.
Beyond CDI, SCFA restoration has implications for gut barrier function, immune regulation, and inflammation that extend to IBD, IBS, and metabolic conditions.
Immune Modulation After FMT
The microbiome profoundly shapes both innate and adaptive immune responses in the gut, and restoration of the microbiome through FMT has measurable immunological consequences.
In CDI specifically, C. difficile toxins drive a pro-inflammatory cytokine cascade (IL-1beta, IL-6, TNF-alpha) that contributes to the severity of colitis.
FMT resolution of CDI is associated with reduction in these inflammatory markers as the epithelial barrier repairs.
Regulatory T cell (Treg) induction:
Multiple commensal bacterial species, particularly from Clostridia class IV and XIVa (many of which are produced in the gut in the presence of specific bile acids and SCFAs), are potent inducers of colonic Tregs.
Treg deficiency is a feature of both CDI and inflammatory bowel disease.
FMT-mediated restoration of these Treg-inducing commensals may contribute to both CDI cure and the partial efficacy signal seen in IBD trials.
FXR pathway activation:
Successful FMT for CDI is associated with increased circulating fibroblast growth factor 19 (FGF-19), consistent with upregulation of the farnesoid X receptor (FXR)/FGF19 pathway. R
Ileal FXR activation causes negative feedback on hepatic bile acid synthesis, reducing primary bile acid secretion into the gut and further lowering the C. difficile germination signal.
FXR agonism also reduces colonic inflammation through mechanisms independent of bile acid homeostasis.
This cascade (microbial restoration leads to secondary bile acid production, secondary bile acids activate FXR, FXR reduces primary bile acid synthesis and reduces inflammation) represents a self-reinforcing loop that explains the durability of FMT responses.
Delivery Methods: Colonoscopy, Capsules, Enema
FMT can be delivered through multiple routes, each with tradeoffs: R
Colonoscopy:
The most studied delivery method. Material is instilled at the level of the ileocecal valve during a standard colonoscopy following bowel prep. The bowel prep eliminates most of the recipient's remaining microbiome, theoretically reducing competition for the incoming donor microbiota. Colonoscopy delivery allows visualization of the colon (identifying colitis severity, pseudomembranes) while delivering material to the proximal colon where much of the therapeutic action occurs. Success rates for recurrent CDI via colonoscopy are approximately 85-95% in most series. Limitations: requires specialist access, is invasive, carries standard colonoscopy risks, and requires sedation.
Oral capsules (frozen or lyophilized):
Multiple preparations of encapsulated frozen or lyophilized FMT have been developed and tested. Capsules are non-inferior to colonoscopy delivery for recurrent CDI in multiple trials. They do not require bowel prep, can be self-administered, and are far more accessible. The FDA-approved product Vowst is an oral capsule formulation.
Enema:
Lower bowel delivery only; less reach than colonoscopy. Efficacy rates are somewhat lower than colonoscopy for CDI (approximately 70-80% versus 85-95%). Lower preparation burden, lower risk.
Nasogastric or nasojejunal tube:
Upper GI delivery; primarily used in severely ill patients who cannot undergo colonoscopy. Carries aspiration risk. Less commonly used now that capsule options are available.
FDA-Approved Products: Rebyota And Vowst
The FDA approval of two standardized FMT-derived products in 2022-2023 represents the transition from procedure-based FMT toward regulated biologic drugs. R
Rebyota (fecal microbiota, live-jslm):
Approved November 2022. A single-dose, rectally administered product derived from donor stool. Contains a broad consortium of donor-derived bacteria in a suspension. Approved for prevention of recurrent CDI in adults 18+ following completion of antibiotic treatment for recurrent CDI. NOT approved for treatment of active CDI. Success rate in pivotal trial: approximately 70.6% success (defined as no CDI recurrence at 8 weeks), with sustained response of approximately 90% at 6 months in those who achieved initial cure. Administered in a clinical setting.
Vowst (fecal microbiota spores, live-brpk):
Approved April 2023. An orally administered product (4 capsules once daily for 3 days) derived from donor stool-derived Firmicutes spores. Firmicutes spores are selected because they are particularly tolerant of the manufacturing process (freezing, lyophilization), standardizable, and are the class of bacteria most critical for secondary bile acid production. Approved for the same indication: prevention of recurrent CDI in adults 18+ following antibiotic treatment. Success rate in pivotal trial: approximately 67.7% success at 8 weeks. Can be self-administered at home after a health care provider dispenses the prescription.
Important limitations of both products:
Neither is approved for treatment of active severe or fulminant CDI. Neither is approved for children. Neither is approved for IBD, IBS, or any non-CDI indication. Both are indicated for prevention of recurrence after antibiotic treatment, not as primary CDI treatment.
The AGA 2024 guideline notes these products do not cover all clinical scenarios and preserves a role for conventional FMT in severe or fulminant CDI not responding to antibiotics. R
Efficacy For Recurrent C. difficile: What The Numbers Say
The evidence base for FMT in recurrent CDI is stronger than for any other indication by a considerable margin.
Meta-analysis and systematic review data:
A 2020 systematic review and meta-analysis published in eClinicalMedicine pooled data from multiple RCTs and found FMT superior to standard antibiotic therapy for recurrent CDI, with absolute benefit estimates showing approximately 305 more per 1,000 patients with CDI prevented compared with control. R
Individual colonoscopy-delivered FMT series consistently report 85-95% cure rates after one or two procedures.
The AGA 2024 clinical practice guideline:
Provides a strong recommendation for FMT-based therapies (including Rebyota and Vowst) to prevent recurrent CDI in immunocompetent patients who have had at least one CDI recurrence. R
Makes a conditional recommendation for conventional FMT in hospitalized adults with severe or fulminant CDI not responding to antibiotics within 2-5 days of starting standard therapy.
Recommends against FMT for IBD or IBS outside of clinical trials.
Honest caveat: one negative trial:
A 2025 Veterans Affairs RCT published in Clinical Infectious Diseases tested capsule-delivered FMT versus placebo in Veterans with recurrent CDI following antibiotic response and found NO difference in recurrence rates. R
This was surprising given the prior positive trials and deserves honest acknowledgment.
Possible explanations include the specific patient population (VA patients with high comorbidity burden), the capsule formulation used, the timing of FMT relative to antibiotic completion, and the definition of recurrence used.
This trial does not overturn the overall evidence base, but it does suggest that FMT in certain populations and delivery contexts may not perform as expected and that the evidence is not uniformly positive.
FMT For IBD: Ulcerative Colitis And Crohn's
IBD represents the most active investigational frontier for FMT outside of CDI.
The rationale is compelling: dysbiosis is a feature of both ulcerative colitis (UC) and Crohn's disease, with reduced diversity and depletion of specific beneficial genera including Faecalibacterium prausnitzii and Roseburia.
What the data shows for ulcerative colitis:
Multiple small RCTs have been conducted. Aggregate data from 9 RCTs (pooled analysis) showed that FMT was superior to placebo for inducing clinical remission in mild-to-moderate UC. Remission rates with FMT in these trials ranged from 24-32% versus approximately 5-9% for placebo/sham.
These are not high absolute numbers, but they are statistically significant signals.
Maintenance of remission after FMT induction in UC has been more difficult to demonstrate.
A Cochrane review found FMT did not significantly improve maintenance of clinical or endoscopic remission in UC. R
Several additional factors appear to influence UC outcomes: anaerobic processing of donor stool may improve efficacy (by preserving obligate anaerobes that are killed by oxygen exposure), higher FMT dosing protocols (more frequent infusions) produce higher remission rates, and donor selection appears to matter.
The "super-donor" phenomenon:
Some donors produce stool that achieves remission in UC recipients at rates far above the mean; other donors produce stool that performs at or below placebo.
This donor-specific effect strongly suggests that specific microbial species or communities, rather than generic microbiome diversity, are driving efficacy in UC.
Identifying the relevant species remains the central challenge for IBD.
Crohn's disease:
Evidence is more limited. Small studies show some benefit in luminal Crohn's, but evidence quality is low and there is no RCT data comparable to the UC literature.
Current clinical guidance:
Both the AGA and ACG recommend against FMT for IBD outside of clinical trials. This is not a statement that it doesn't work; it is a statement that the evidence is not yet sufficient for routine clinical use and that standardization remains poor.
FMT For IBS, Metabolic Disease, And Other Indications
IBS:
Pooled RCT data for FMT in IBS shows no significant improvement in overall IBS symptoms at 12 weeks. R
There is high heterogeneity between studies. Subgroup analysis suggests that FMT delivered via upper GI route (duodenoscopy or nasojejunal) may reduce IBS severity compared with placebo, but this is not a robust enough finding for clinical recommendations.
AGA recommends against FMT for IBS outside of clinical trials.
Metabolic syndrome, obesity, and NAFLD:
Gut microbiome dysbiosis is documented in metabolic disease. Animal model data shows that FMT from lean donors can improve insulin sensitivity in obese animals. Small human studies show transient improvements in insulin sensitivity and lipid profiles. Effects have not been durable in most human trials. No FMT product is approved or clinically recommended for metabolic indications.
Neuropsychiatric conditions:
The gut-brain axis has generated substantial interest. FMT is being investigated for major depressive disorder (through inflammatory and serotonin signaling mechanisms), autism spectrum disorder, Parkinson's disease, and Alzheimer's disease. These remain early-stage with no RCT-level evidence sufficient for clinical guidance.
Multidrug-resistant organism (MDRO) decolonization:
One of the more mechanistically plausible emerging indications. A randomized placebo-controlled trial found that while FMT initially caused low-level transfer of antibiotic resistance genes from commensal bacteria, it was ultimately followed by long-term protection against new antibiotic resistance genes as stable microbial communities formed. R
Randomized trial evidence from Israel showed that FMT reduced VRE and CPE carriage in hematopoietic stem cell transplant recipients.
This remains investigational.
Immune checkpoint inhibitor colitis:
Case series report clinical improvement in immune-related colitis refractory to steroids and biologics in cancer patients on checkpoint inhibitor therapy. The mechanistic rationale is sound (restoring microbial regulation of mucosal immune responses). Larger trials are needed.
Donor Selection And Screening
The donor is the single most important variable in FMT outcome after delivery method.
Standard donor screening includes: R
Clinical history exclusions:
- Active gastrointestinal disease or symptoms
- Recent antibiotic use (typically within 3-6 months)
- Known inflammatory bowel disease, irritable bowel syndrome, or functional GI disorders
- Recent travel to areas with high endemic pathogens
- High-risk behaviors for bloodborne infection
- Immunocompromising conditions
- Recent gastrointestinal procedures
- Obesity (BMI above 30 in some programs, due to metabolic transfer concerns)
Laboratory testing of donors:
Serologic and stool testing for pathogens including: C. difficile (the intended target, must be absent in donor), Hepatitis A, B, C, HIV 1 and 2, HTLV 1 and 2, Syphilis, Enteric pathogens (Salmonella, Campylobacter, Shigella, E. coli O157:H7, Yersinia, Cryptosporidium, Giardia, Cyclospora, Isospora), Norovirus, Extended-spectrum beta-lactamase producing Enterobacteriaceae (ESBL), Vancomycin-resistant Enterococci (VRE), Carbapenem-resistant Enterobacteriaceae (CRE), and Methicillin-resistant Staphylococcus aureus (MRSA).
After the COVID-19 pandemic, SARS-CoV-2 testing of donors and stool was added by most programs.
The screening burden is substantial: most commercial stool bank programs historically rejected approximately 95% of potential donors based on these criteria.
The "super-donor" concept:
Beyond safety screening, there is increasing interest in selecting donors based on their specific microbial community composition, particularly for non-CDI indications where specific species appear to drive efficacy.
For IBD, donors with high levels of Ruminococcaceae and Lachnospiraceae and abundant secondary bile acid production capacity may be preferentially effective.
Safety: Real Risks And Reported Deaths
FMT is not without serious risk, and honest communication of those risks is important.
Common adverse events (mild, transient):
Most adverse events from FMT are gastrointestinal and resolve within 24-48 hours: diarrhea, flatulence, abdominal cramping, bloating, nausea. These are reported in the majority of recipients and are considered procedure-related rather than indicative of harm.
Rare but serious adverse events:
The most significant documented safety events involve transmission of pathogenic organisms from donor to recipient.
2019 ESBL event: Two immunocompromised patients developed invasive ESBL-producing E. coli infections following FMT from the same donor whose stool was not tested for ESBL; one patient died. R
This prompted the FDA to mandate ESBL, VRE, CRE, and MRSA testing for all investigational FMT.
2020 STEC/EPEC event: Six patients who received FMT from a US stool bank developed enteropathogenic E. coli (EPEC) or Shiga toxin-producing E. coli (STEC) infections. R
Two patients died, though STEC infection as the direct cause of death was not confirmed because specimens were not collected prior to death.
The stool bank involved had not tested for EPEC because EPEC prevalence in healthy asymptomatic adults was considered too low to warrant routine screening.
What these events mean practically:
FMT-related serious adverse events are rare when appropriate donor screening is performed. The patients who died were immunocompromised and receiving investigational FMT through stool bank products that lacked the full screening now required. FMT via the FDA-approved products (Rebyota and Vowst) uses standardized manufacturing with comprehensive testing. Conventional FMT in immunocompetent patients from adequately screened donors has a strong safety record in clinical series. The risk is meaningfully higher in immunocompromised patients (solid organ transplant recipients, hematologic malignancy, patients on biologics) and this population requires extra caution, more rigorous donor screening, and careful risk-benefit discussion.
The OpenBiome Collapse And The Regulatory Transition
OpenBiome was the primary US stool bank supplying conventional FMT product for most of the country for over a decade.
It provided processed, screened donor stool to hospitals and gastroenterologists operating under FDA enforcement discretion, meaning the FDA chose not to enforce investigational new drug (IND) requirements for conventional FMT used to treat C. difficile not responding to standard therapies.
This enforcement discretion created an accessible middle ground between regulated drug and informal procedure.
After the FDA approved Rebyota in November 2022, it discontinued enforcement discretion for centralized stool bank distribution.
In August 2024, the FDA conducted an unannounced inspection of OpenBiome and the University of Minnesota's microbiota therapeutics program. No safety concerns were raised, but FDA inspectors stated that continued distribution required operating under an IND.
OpenBiome and the University of Minnesota voluntarily discontinued distribution shortly after. OpenBiome subsequently announced it would cease operations entirely.
The result: a significant reduction in access to conventional FMT for patients with severe or fulminant CDI who are not candidates for the approved products (which are indicated only for recurrent CDI in outpatients, not for severe or fulminant inpatients). R
The AGA sent a letter to the FDA in October 2024 urging preservation of access to conventional FMT for patients where approved products are not appropriate.
The regulatory situation as of 2025-2026 remains unsettled, with conventional FMT increasingly restricted to clinical trials or hospital-operated programs operating under IND, while the approved products cover outpatient recurrent CDI and leave gaps in care for inpatient severe disease.
What To Stay Away From
- DIY FMT (at-home self-administered FMT from an unscreened donor): donor screening is not optional; the safety events described above involved institutional FMT from stool banks with partial screening and well-resourced laboratory infrastructure; unscreened donors carry unknown pathogen risk including ESBL organisms, STEC, hepatitis, HIV, Norovirus, and parasites; the internet-based DIY FMT community operates without these safeguards and the risk-benefit calculation is substantially less favorable than clinical FMT
- FMT for conditions where evidence does not support benefit: IBS, obesity, and neuropsychiatric conditions remain investigational; receiving FMT for these indications outside of a clinical trial means accepting real pathogen transmission risk without the oversight or evidence base that would justify it
- Skipping antibiotic treatment before FMT for active CDI: FMT is approved and indicated for PREVENTION of recurrence after antibiotic treatment, not as a primary treatment for active CDI; standard-of-care antibiotics (vancomycin or fidaxomicin) must complete the course first
- Assuming stool bank products are equivalent to the FDA-approved biologics: Rebyota and Vowst have passed the FDA's manufacturing and safety standards; stool bank products vary in processing, anaerobic handling, storage conditions, and screening depth; not all FMT products are equivalent
- Failing to disclose immunocompromised status before FMT: the risk of serious adverse events from FMT is substantially higher in immunocompromised patients; this population requires extra donor screening, different risk-benefit discussions, and should generally be treated at centers with experience in high-risk FMT
Testing
C. difficile toxin PCR or GDH/toxin combination assay: Required before any FMT consideration. Active CDI must be confirmed. Testing should also be performed at the time of suspected recurrence (at least 2 weeks after prior episode and after completion of antibiotic therapy).
Comprehensive Stool Analysis: Broad dysbiosis evaluation. Not required for CDI FMT decisions, but useful for understanding the baseline microbial state and potentially relevant for non-CDI indications where the underlying dysbiosis pattern matters. Can identify ongoing pathogen burden, opportunistic infections, inflammation markers (calprotectin), and short-chain fatty acid producers.
Fecal calprotectin: Marker of intestinal inflammation. Elevated in active CDI, IBD, and colorectal cancer. Useful to monitor recovery after FMT: falling calprotectin tracks resolution of mucosal inflammation. Relevant in FMT for IBD trials as an outcome measure.
Organic acids test (OAT): Indirectly reflects microbial metabolite production. Can show SCFA production signatures and pathogen-associated metabolites. Elevated D-arabinitol (yeast), indican (tryptophan dysbiosis), and certain organic acid patterns suggest ongoing dysbiosis after FMT that may not be apparent on standard stool testing.
CBC with differential, CMP: Active CDI can cause significant leukocytosis (white count above 15,000 is a marker of severity), acute kidney injury, and electrolyte disturbances from diarrhea. Monitoring these markers before FMT assesses disease severity; fulminant CDI (leukocytosis above 30,000 or rising creatinine) may require surgical consultation alongside FMT.
Mechanisms Of Action
Simple:
- FMT works because C. difficile infection is fundamentally an ecological collapse problem, not just an infection problem; antibiotics wipe out the diverse microbial community that would normally prevent C. difficile from taking hold, and antibiotics alone cannot restore that community; FMT reintroduces a functioning ecosystem that can displace C. difficile by restoring the metabolic and competitive conditions that kept it suppressed.
- The most important thing FMT brings back is a group of bacteria that convert the bile acids in your colon from ones that tell C. difficile spores to "wake up and grow" into ones that tell them to "stay dormant"; this bile acid shift is the central mechanism by which FMT breaks the recurrence cycle.
- Donor microbiota also outcompete C. difficile for nutrients, produce chemicals (butyrate, propionate, acetate) that maintain the gut lining and suppress pathogens, and re-establish the immune tone of the colon in ways that make it less hospitable for opportunistic infections.
- The FDA-approved products (Rebyota and Vowst) are standardized versions of FMT: Rebyota is a broad donor stool preparation given rectally, Vowst is an oral capsule containing only the spore-forming bacteria from donor stool, since those are the specific organisms responsible for restoring bile acid chemistry.
- FMT does not work for everything: for diseases like ulcerative colitis where the dysbiosis is more complex and overlaps with immune dysfunction, FMT produces remission in roughly 1 in 4 or 1 in 3 patients versus 1 in 20 for placebo; it works in some patients but not others, and we do not yet know how to predict who will respond.
Advanced:
- The bile acid-germination axis and colonization resistance restoration: C. difficile spore germination is an exquisitely regulated process triggered by specific bile acid species. Taurocholate (TCA, a conjugated primary bile acid) is the canonical germinant; it binds to the germination receptor CspC in the inner membrane of the spore. Glycine acts as a co-germinant through a separate mechanism. In the antibiotic-depleted gut, BSH-producing Lachnospiraceae and Ruminococcaceae are absent; TCA remains unconjugated, accumulates, and provides abundant germination signal. After FMT, BSH-expressing Lachnospiraceae colonize rapidly (often within 24-48 hours post-FMT), deconjugating bile acids. Bacteria encoding the bai operon (including Clostridium scindens) then 7alpha-dehydroxylate primary bile acids to DCA and LCA, which directly inhibit vegetative C. difficile growth by multiple mechanisms including disruption of cell membrane integrity, inhibition of sporulation, and suppression of toxin A and B expression. The entire bile acid chemistry of the colon shifts from a pro-germination to an anti-germination state within days, explaining the rapid resolution of CDI symptoms typically observed within 48-72 hours of a successful FMT. R
- SCFA production, epithelial repair, and Treg induction: Butyrate produced by fermentative commensals (primarily Faecalibacterium prausnitzii, Roseburia intestinalis, and other Clostridia class IV/XIVa) serves three distinct functions post-FMT. First, butyrate is the primary energy substrate for colonocytes, driving ATP production via beta-oxidation; in CDI, colonocyte energy failure from toxin-mediated disruption is compounded by the absence of butyrate, and restoration of butyrate supply supports epithelial repair. Second, butyrate inhibits histone deacetylases (HDACs) in colonic lamina propria, leading to increased histone acetylation at FOXP3 loci in naive T cells, promoting their differentiation into Foxp3+ regulatory T cells (Tregs). Colonic Tregs suppress effector T cell activation and maintain immune tolerance to commensal bacteria; their depletion in CDI and IBD contributes to the inflammatory pathology of both conditions. Third, butyrate directly suppresses NF-kB signaling in colonocytes, reducing IL-8 production and neutrophil recruitment. R
- The super-donor phenomenon and donor selection for IBD: The observation that specific donors produce dramatically superior remission rates in UC trials (remission rates of 40-50% from "super-donors" versus single-digit rates from average donors) has driven a molecular search for the critical community members. Analysis of super-donor microbiomes from multiple trials has identified consistent enrichment in specific genera: Ruminococcus gnavus, Blautia, Lachnospiraceae, and Eubacterium hallii. These bacteria share two properties: they produce high levels of butyrate and they express bile salt hydrolases and 7alpha-dehydroxylases, suggesting that the same bile acid metabolism and SCFA machinery critical for CDI is also the relevant therapeutic signal in IBD, though the immunological targets differ.
More Research
- FMT for recurrent CDI achieves 80-90% cure rates across most well-conducted series using colonoscopy delivery, making it the most effective intervention in the CDI treatment armamentarium; the 2020 systematic review and meta-analysis found approximately 305 more CDI recurrences prevented per 1,000 patients treated compared with control, with no increase in serious adverse events in properly screened and selected patients. R
- The FDA approval of Rebyota (November 2022) and Vowst (April 2023) represents the first time microbiome-derived products have received full biologic drug approval in the US; both are indicated only for prevention of recurrent CDI in outpatient adults following antibiotic treatment, not for active CDI treatment, not for IBD, and not for pediatric use; this leaves significant gaps in care, particularly for severe and fulminant inpatient CDI. R
- Donor-specific factors, particularly the abundance of bile salt hydrolase-encoding and bai-operon-encoding bacteria, predict FMT success for both CDI and IBD better than overall microbial diversity metrics; this is the scientific basis for the "super-donor" phenomenon and is driving the development of defined live biotherapeutic products (LBPs). R
- Safety risks from FMT are real and must be disclosed: the 2019 ESBL transmission event resulting in one patient death and the 2020 STEC/EPEC events from a US stool bank established that inadequate donor screening can result in fatal pathogen transmission; the patients who died were immunocompromised, reinforcing that immunocompromised recipients require extra caution. R
- The collapse of OpenBiome and the FDA's enforcement posture effectively ending the stool bank model for conventional FMT in the US has created a practical access crisis for patients with severe or fulminant CDI who need FMT and cannot use the approved products. R
Jacob Gordon
INHC, FMT-C
Board Certified Health Coach
I spent years battling unexplained chronic illness before discovering biohacking, epigenetics, and functional medicine. Now I share that research at MyBioHack to help others find their own answers.
Book a ConsultationRelated Protocols & Supplements
Deep-dive chapters and recommended supplements for this topic
Spore-Based Probiotics
1 cap with food
L-Glutamine
5g 2x/day on empty stomach
Butyrate
300mg 2x/day with meals